-
THE KNEE AND ANKLE IN CEREBRAL PALSY
Dr. Ashok N. Johari
Paediatric Orthopaedic Surgeon
President, POSI
INTRODUCTION
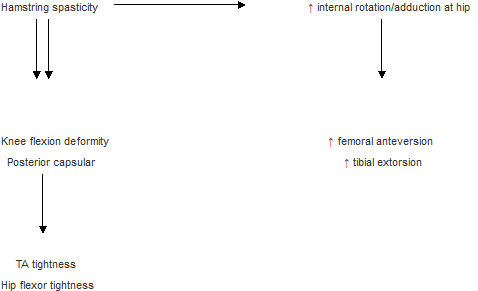
Knee and ankle problems in cerebral palsy cannot be isolated from the hip and pelvis as each body segment has an interaction with the other. This happens because of mechanical variations in muscle length and tension resulting from changes in spatial positioning of the extremity segments.
Amongst other factors, functional deficits in cerebral palsy patients result from the following:
- Spasticity with resultant contractures of a dynamic or static nature.
- Weakness or lack of power generation caused by a lack of sarcomeres or because of altered biomechanics due to a ‘lever arm dysfunction’. Examples of lever arm dysfunction include knee extensor weakness resulting from external tibial torsion and an abducted planovalgoid foot.
- Lack of voluntary control gives rise to mass patterns of movement, compensatory mechanisms, and gait deviations.
1, 2 and 3 above cause a change in the agonist-antagonist balance giving rise to deformities and further skeletal problems.
Orthopaedic evaluation in cerebral palsy related to the knee and ankle
- Spasticity is graded on the Ashworth scale1. The Tardieu scale2 is very useful to evaluate ‘dynamic’ spasticity arising from a changing stretch velocity. R1 is the point where a catch is felt on rapid movement of the affected part. R2 is the point where a catch is felt on slow stretch. The difference tetween R1 and R2 (R2 – R1) signifies the dynamic component of spasticity which could respond to different modalities of treatment like botulinum toxin or therapy.
- Deformities and range of motion of different joints are recorded like for other orthopaedic disorders. The patient has to be as relaxed as possible.
- Weakness is graded on the MRC scale. All major muscle groups are examined.
- Lack of selective motor control signifies severity of involvement. With severe impairment, voluntary control is lacking. Selective motor control can be tested by relaxing the antagonist and testing agonist function3.
- Static alignment of the lower limb – evaluation of torsion and angular deformity, patellar position, foot alignment etc.
- Special tests suggesting tightness of muscle groups include the Thomas test (hip flexon), Ely’s test (rectus femoris), popliteal angle (hamstrings) and Silverskiold test (gastrocnemius).
- The gait cycle is carefully evaluated looking at each of the phases – stance and swing. Segment positioning is noted during the double limb support and single leg stance. A careful note is made of the hip-knee-ankle and foot interactions.
FOOT AND ANKLE IN CEREBRAL PALSY
The different foot and ankle problems in cerebral palsy are
- Equinus
- Calcaneus
- Equino varus
- Equino valgus
Equinus
In the assessment of a patient who has equinus it is most important to ascertain if the equinus is apparent or real. Apparent equinus (Fig.1) is secondary to a knee/hip flexion deformity. Careful observation in gait and clinical examination would show that the ankle and foot is in a neutral position as opposed to a true equinus in which it remains plantar flexed throughout the gait cycle.
The Tardieu scale is perhaps one of the best modalities of assessment as dynamic spasticity would need plasters or botulinum. Power of the antagonists i.e. dorsilflexors is to be assessed. After correction of the equinus if the dorsiflexors are poor, the patient will have a drop foot gait. It is important to assess the situation at the knee and hip as this may require simultaneous correction. Presence of hamstring spasticity which is not tackled during a TA lengthening can create a crouch.
Compensatory mechanisms for an equinus deformity include knee hyperextension and a forward trunk lean or knee and hip flexion (Fig.2). It is also important to know that the natural history of an equinus foot in spastic diplegia is reversal of the deformity into a calcaneus with growth and hence one has to be cautious about early lengthening of the T.A. in isolation.
In the management of equinus the following modalities can be used:
i) Physiotherapy and Splintage
An AFO is the commonest type of splint used to control equinus. An articulated AFO allows dorsiflexion but prevents plantarflexion. This can be used where the dorsiflexors are fairly strong and allows a more natural gait.
ii) Plasters
Single or serial casting is of help for mild to moderate degrees of TA contracture. Inhibitory cast help reduce the muscle tone.
iii) Botulinum toxin4
Botulinum toxin causes a blockade in the transmission of acetylcholine at the neuromuscular junction. This reduces spasticity. Reduction of spasticity prevents deformity and wrong patterns of use of the extremity. Botulinum works very well for dynamic spasticity. Along with casting it can be used to manage mild to moderate contractures of the TA’s.
iv) Surgery
Severe deformity requires surgery. This has always to be approached with caution as complications are common. Underlengthening gives rise to recurrence of the deformity while overlengthening causes a calcaneus which is a bigger functional problem.
An analysis of the risk factors in isolated calf lengthening in cerebral palsy5 revealed an incidence of 22% of recurrent equinus and a 36% incidence of calcaneus at a 5 to 10 year follow-up. Children with diplegia who had surgery when aged 8 years or less had a 44% risk of calcaneus, while those over 8 years had a 19% risk. In hemiplegia, the incidence of recurrent equinus was 38% and only 4% developed calcaneus. An increased severity of involvement, female gender, age at operation of less than 8 years and lengthening of the TA were risk factors for calcaneus. Hemiplegia, males and an aponeurotic muscle lengthening increased the risk of recurrent equinus.
Techniques of lengthening the TA include the following
- Aponeurotic – gastrocnemius recession ( Strayer’s6, Baumann7)
- Aponeurotic – gastrocnemius plus soleus ( Baker’s8, Vulpius9)
- Tendon lengthening – (Hoke’s10, White’s11) or a Z lengthening
- Translocation of the tendo Achilles (Murphy12)
Other less common techniques of lengthening / reducing spasticity in the gastrocnemius include
- Partial neurectomy of the gastrocnemius13
- Lengthening of the origin of gastrocnemius14
The Silverskiold test helps differentiate between tightness of the gastrocnemius vs. gastrosoleus.
Effects of TA lengthening on the knee and hip have to be considered. In the presence of spastic hamstrings, coupled with a loss of the extension couple because of lengthening of the TA, a crouch results. Similarly, a flexion contracture of the hip can cause a forward lean of the trunk even though the foot may become plantigrade.
Equinovarus
This is caused by an imbalance between the invertors and evertors. A subtle posturing of the foot if unchecked eventually gives rise to a bony deformity.
In the clinical examination it is important to note whether the varus appears only in the swing phase, suggesting tibialis posterior overactivity. This is more so if the tibialis anterior is weak. Also a note is made of the correctibility of the foot. A fixed deformity indicates a myostatic contracture which needs a lengthening of the shortened tendon.
Split transfers are of great benefit in preventing over correction. For a spastic tibialis anterior a split transfer is done to the lateral side (SPLATT15). Tibialis posterior overactivity needs an intramuscular lengthening (Frost16) if the imbalance is mild or a split transfer to the peroneii if the imbalance is greater and the peroneii are weak. (SPOTT17) A shortened tibialis posterior may need to be Z lengthened precluding transfer. In this situation I often isolate the tibialis posterior further ahead on the cuneiform taking its periosteum and then split the tibialis for transfer. This allows a relative lengthening of the tibialis posterior to be accomplished along with the transfer. A TA lengthening in some form is usually necessary for a contracture. Sometimes bony procedures like a metatarsal osteotomy or a Dilwyn Evans procedure (lateral column shortening) may be needed for an advanced case. Osteotomy of the os calcis is also an option for the heel varus. A triple arthrodesis is reserved as a salvage procedure.
Spastic valgus foot
This is the commonest deformity in spastic diplegia. Weak invertors coupled with a tight TA gives rise to evertor overactivity and a midtarsal break. The forefoot abducts and everts and the invertors fail. Eventually bony deformities develop. There is a lengthening of the medial column and a shortening of the lateral one. Associated findings may include an internal femoral torsion, tight hamstrings and adductors and an external tibial rotation.
Surgical management may demand a peroneal lengthening, medial talonavicular reefing and tibialis posterior advancement and a lateral column lengthening – the so called Mosca’s procedure18. Occasionally a Grice’s procedure or its variant may be needed for a fairly severe heel valgus. Osteotomies are an option and a triple arthrodesis is the last resort. If ankle valgus exists, a supramalleolar osteotomy may be needed.
Calcaneus
This is identified by dorsiflexion of the foot throughout stance especially at midstance. Presence of calcaneus causes excessive hip and knee flexion in gait. The contra lateral step length is reduced along with a reduction in ipsilateral single stance phase. Increased demands are put on the quadriceps. More often than not as mentioned earlier, calcaneus gait is iatrogenic and due to isolated heel cord lengthenings.
Rectification of a calcaneus foot is difficult. A floor reaction orthosis (FRO) may benefit by allowing the foot to be held plantigrade. A rear entry hinged FRO is helpful. Surgical options have limitations and may include tendon transfers or heel cord tenodesis and calcaneal osteotomies. Proximal surgery may be necessary in this situation.
KNEE PROBLEMS IN CEREBRAL PALSY
Corollary
Besides hamstring lengthenings, TA lengthening, hip flexor release, knee capsular release and femoral, tibial derotation osteotomies may be needed.
Knee problems in cerebral palsy19 include
- Crouch gait
- Jump knee gait
- Stiff knee gait which may be a feature in isolation or with a crouch or jump knee gait
- Recurvatum knee gait
In diplegia what starts off as a tight TA gradually progresses to a crouch gait (Fig.3) along with foot dorsiflexion and break of the foot at the midtarsal level and a flexed knee. Very often a crouch gait is secondary to overlengthening of the TA.
Undetected hip flexion contracture may be a part of the cause or effect cycle responsible for crouch. This should always be looked for.
Milder degrees of crouch can be manged by a FRO (floor reaction orthosis) along with physiotherapy – hamstring stretching and quadriceps strengthening exercises. More severe crouch needs botulinum injection for the hamstrings and hip flexors and casting above the knee to stretch the tight hamstrings. Correction can then be maintained with a FRO.
Surgery is need for cases which do not respond conservatively. Hamstring lengthening is required and most often the medial hamstrings are tackled by way of aponeurotic lengthening of the semi membranosus and Z lengthening for the semitendinosus and gracillis. If the hip flexors are tight an intramuscular psoas release is carried out. A tight rectus femoris may be released proximally or transferred to the semitendinosus for a better knee flexion in swing20. A transfer may not be possible if there is a large flexion deformity of the knee.
If the flexion deformity of the knee exceeds 30°, a knee capsulotomy or recurvatum osteotomy is advisable. This may be combined with a patellar advancement.
Along with hip and knee flexion if the foot has an equinus deformity the centre of the knee is placed higher and the patient ‘jumps’ or vaults over the knee in gait (Fig.4). This gives rise to a jump knee gait more common in diplegics. Stiffness at the knee can be a component of this gait pattern.
Non-operative options of management would include physiotherapy and serial casting, AFO’s and use of botulinum at multiple levels. Surgical correction would demand a simultaneous correcton at all levels including the ankle, knee and hip. If stiff knee is a feature, a rectus transfer to the hamstrings may be needed.
Stiff Knee
Co-spasticity in the hamstrings and rectus femoris or quadriceps causes a stiffness of the knee in gait with a reduced excursion of the hip and knee in swing. This gives rise to impaired foot clearance and compensatory movements of circumduction and external rotation and contralateral vaulting. Rectus femoris tightness is demonstrated statically by the Ely’s test and dynamically by a reduced swing of the knee. In this situation just releasing the hamstrings will aggravate extensor spasticity causing the knee to stiffen in extension. The weak hamstrings are unable to flex the knee against the now stronger quadriceps. Hence for a stiff knee, simultaneous relaxation of the hamstrings and quadriceps is required. This is most commonly achieved by hamstring elongation with release of the direct head of rectus femoris or transfer of the rectus femoris to the semitendinosus which increases swing as compared to a release of the rectus itself. A transfer is advocated if the preoperative range of motion is less than 80% of normal.
A recurvatum knee is secondary to tightness of the gastrosoleus (Fig.5). Sometimes this may be a complication of releasing the hamstrings when the exact nature of spasticity of the quadriceps is not understood.
Conservative measures include use of a solid or articulated AFO to keep the tibia on the foot and prevent it from hyperextension. Botulinum can be used in addition to casting or therapy to relax the gastrosoleus. In some cases a TA lengthening may be necessary in addition to a rectus release or transfer.
TORSIONAL PROBLEMS AND LEVER ARM DYSFUNCTION21
Torsional problems commonly seen in cerebral palsy are an internal femoral torsion and external tibial torsion. This is accentuated in diplegics by external rotation and mid foot break occurring at the foot level. To gain back the most effective muscle action, skeletal lever realignment becomes mandatory if the existing malalingment is significant. This may demand an external rotation femoral osteotomy with an internal rotation tibial osteotomy and a foot reconstruction. A CT scan helps to evaluate the rotational profile.
GAIT PATTERNS IN SPASTIC HEMIPLEGIA AND DIPLEGIA
Gait patterns in spastic hemiplegia have been described by Winters et al22 (Fig.6). Their type 1 is a drop foot because of weak dorsiflexors with no contracture of the TA. In type 2A there is a true equinus but with a neutral knee and extended hip. In type 2B there is a true equinus with a recurvatum knee. In type 3 there is a true equinus with a jump knee. This would demand tackling the TA, hamstrings and hip flexors. In cases of cospasticity between the hamstrings and hip flexors, a rectus femoris transfer may be needed. In type 4 hemiplegia there is unilateral severe involvement at the hip, knee and ankle like in a jump gait but with tightness of the hip adductors giving rise to an adducted, internally rotated limb and pelvic retraction. This may require in addition to a hip, knee, ankle surgery an adductor release along with an external rotation osteotomy of the femur.
Gait patterns in spastic diplegia23 (Fig.7) are based on changes taking place at the ankle, Type 1 is a true equinus. Type 2 is a true equinus with knee and hip flexion. This is the classical jump knee gait. Type 3 is hip and knee flexion with the foot at 90° - apparent equinus. Type 4 is a crouch gait with the hip and knee flexed and the foot in dorsiflexion.
Type 3 diplegia with apparent equinus is important to differentiate from the other types as this is the variety in which lengthening of the TA is unnecessarily carried out increasing the crouch and impairing the post operative results.
SINGLE EVENT MULTILEVEL SURGERY (SEMLS)
Very often there is a complex interaction between the hip, knee and ankle in cerebral palsy more so when the involvement is severe. Changing the biomechanical situation in isolation at one of the joints can give rise to problems at other levels eg. heel cord lengthening giving rise to crouch in the absence of treatment for tight hamstrings or hip flexors. Hence a detailed clinical evaluation of the patient is mandatory. Where facilities for instrumented gait anlysis are available, this provides a definite help and picks up aberrations not visible to the clinical eye. Multiple clinical examinations and video gait recordings may help bridge some differences. Great experience is required if one treats these patients on a purely clinical basis keeping in mind all possible interactions.
The great advantage of single day surgery is that the patient needs to be hospitalized once and undergoes a single rehabilitation phase unlike in the past when repeated hospitalization and rehabilitation were required – a term called the ‘birthday syndrome’ by Rang24. SEMLS does mean long surgery and a greater danger of things getting out of hand, especially for inexperienced surgeons, because of unsuspected spasticity or weakness.
REFERENCES :
- Ashworth, B., (1964) Preliminary trial of carisoprodol in multiple sclerosis. Practitioner. 192: 540-542.
- Tardieu G, Shentoub S, Delarue R ( 1954). A la recherche’d’ une technique de mesure de las spasticite. Revue Neurologique 91:143-144. Quoted in Boyd R, Graham HK (1999b). Objective measurement of clinical finding in the use of botulinum toxin type A for the management of children with cerebral palsy. Eur J Neurol 6: S23-S35.
- Boyd R, Graham HK (1999b).Objective measurement of clinical finding in the use of botulinum toxin type A for the management of children with cerebral palsy. Eur J Neurol 6:S23-S35.
- Boyd R, Graham HK (1999b)Botulinum toxin type A for the management of children with cerebral palsy: Indications and outcome. Eur J Neurol 4:S15-S22.
- Borton DC, Walker K., Pirpiris M, Nattrass GR, Graham HK (2001). Isolated calf lengthening in cerebral palsy. Outcome analysis of risk factors. J Bone Joint Surg. 8.3-B: 364-370.
- Strayer LM Jr. (1950). Recesion of the gastrocenemius: an operation to relieve spastic contracture of the calf muscles. J Bone Joint Surg. 32-A: 671-676.
- Baumann JU, Koch HG. (1992). Lengthening of the anterior aponeurosis of musculus gastrocnemius through multiple incisions. Orthopaedics and Traumatology. 1(4): 278-282
- Baker LD. (1954). Triceps surae syndrome in cerebral palsy. Arch Surg. 68:216-221.
- Javors JR, Klaaren HE. (1987). The Vulpius procedure for correction of equinus deformity in cerebral palsy. J. Pediatr Orthop. 7: 191-193.
- Hatt RN, Lamphier TA. (1947). Triple hemisection: a simplified procedure for lengthening the Achilles tendon. N Engl J Med. 236:166-169.
- White JW. (1943). Torsion of the Achilles tendon: its surgical significance Arch Surg. 46: 784-787.
- Pierrot AH, Murphy GB. (1974). Heel cord advancement: a new approach to the spastic equinus deformity. Orthop Clin North Am. 5: 117-126.
- Phelps WM. (1957). Long-term results of orthopaedic surgery in cerebral palsy. J Bone Joint Surg. 39-A: 53-59.
- Silver CM, Simon SD. (1959). Gastrocnemius-muscle recession (Silverskiold operation) for spastic equinus deformity in cerebral palsy. J Bone Joint Surg. 41-A: 1021-1028.
- Hoffer MM, Barakat G, Koffman M. (1985). 10-year follow-up of split anterior tibial tendon transfer in cerebral palsied patients with spastic equinovarus deformity. J Ped Orthop. 5: 432-434.
- Ruda R, Frost HM (1971). Cerebral Palsy. Spastic varus and forefoot adductus, treated by intramuscular posterior tibial tendon lengthening. Clin Orthopaedics Related Res. 79: 61-70.
- Green NE, Griffin PP, Shivavi R. (1983). Split posterior tibial tendon transfer in spastic cerebral palsy. J Bone Joint Surg. 65-A: 748-754.
- Mosca V. (1995). Calcaneal lengthening for valgus deformity of the hindfoot. J Bone Joint Surg. 77-A: 400-512.
- Sutherland DH, Davids JR (1993). Common gait abnormalities of the knee in cerebral palsy. Clin Orthopaedics Related Res. 288: 139-147.
- Gage JR, Perry J, Hicks RR, Koop S, Werntz JR. (1987). Rectus femoris transfer to improve knee function of children with cerebral palsy. Dev Med Child Neurol 29: 159-166.
- Gage JR. (1991). Gait analysis in cerebral palsy. London: MacKeith Press. 102-107.
- Winters TF, Gage JR, Hicks R. (1987). Gait patterns in spastic hemiplegia in children and young adults. J Bone Joint Surg. 69-A: 467-441.
- Rodda J, Graham HK. (2001). Classification of gait patterns in spastic hemiplegia and spastic diplegia: a basis for a management algorithm. Eur J Neurol. 8 (Suppl. 5): 98-108.
- Rang M. (1990). Cerebral palsy. In : Morrissy, RT, Ed. Lovell and Winter’s Pediatric Orthopaedics, 3rd edn. Philadelphia: JB LIppincott Co., pp. 465-506.
Blount Disease: Management Strategies
Dr Sanjeev Sabarwal
The pathogenesis of genu varum in Blount’s disease is based on the Heuter-Volkman principle of increasing compressive forces causing growth inhibition. Excessive pressure at the proximal medial tibial cartilaginous epiphysis causes altered structure and function of the chondrocytes along with delayed ossification of the epiphyses. Related to the asymmetric growth with relative inhibition of the postero-medial portion of the proximal tibial growth plate, a three-dimensional deformity of the lower leg including varus, procurvatum and internal tibial torsion develops. This entity can lead to progressive deformity with gait abnormality, leg length inequality and premature arthritis of the knee. Standing full-length antero-posterior (AP) radiograph (teleoroentgenogram) of the entire length of both lower extremities with the patella forward is crucial for analysis of frontal plane alignment. Despite being referred to as “tibia vara”, Blount disease may have other sources of medial axis deviation arising from the distal femur and intra-articular deformity creating dynamic varus malalignment. Full-length AP and lateral views of the tibia are needed to fully assess the presence of biplanar deformities in the proximal and distal ends of the tibia.
Since Blount disease affects children, one needs to consider not only the current deformity and leg length discrepancy, but also anticipated discrepancy at skeletal maturity, with and without treatment. The goal of treatment is to attain a normally aligned lower extremity with normal joint orientation and equal leg lengths at skeletal maturity. Besides proximal tibial metaphyseal osteotomy, with either acute or gradual correction, several other realignment strategies are available. These include lateral hemiepiphyseodesis around the knee, distal femoral osteotomy, medial tibial plateau elevation, resection of physeal bony bar and gradual asymmetric proximal tibial physeal distraction. Often, two or more of these surgical modalities are applied at the same time or in a staged manner. Examples include lateral hemi-epiphyseodesis of the proximal tibia and fibula along with medial plateau elevation in a child with severe form of early onset Blount. If associated metaphyseal deformity is also present, one may need to perform a second osteotomy for correction at this site as well as gradual lengthening to equalize limb lengths at maturity. Similarly, an adolescent who has deformity originating at two sites i.e. the distal femur and proximal tibia, may need a two level osteotomy or a combination of osteotomy at one location and lateral hemi-epiphyseodesis at the other. The location and timing for the hemi-epiphyseodesis is based on the magnitude of deformity and growth remaining. The concept of individualizing treatment based on a comprehensive analysis of the limb deformity, amount of growth remaining, psychosocial status of the patient and ability of the surgeon to execute a well outlined treatment plan with precision and safet
-
MODIFIED TRIPLE ARTHRODESIS OF FOOT
DR. AK PANDEY RANCH | INDIA
To combat certain complication (like pseudoarthrosis, painful gait, shortening of foot) of standard Lambrinudi’s triple arthrodesis, the present procedure of modified triple arthrodesis has been tried in 394 feet in an average age of 11.6 years (paralytic foot drop, neglected club foot, cerebral palsy feet) since 29 years with an average followup of more than 3 years
In modified triple arthrodesis steindles calcaneal fasciectomy and/or Achilles tendon lengthening is done through a curved lateral - tarsal incision the subtalar, calcaneocuboid and talonavicular joints are exposed. Sinus tarsi is emptied keeping the foot maximum planter flexed almost lower half of talar head and lower third to fourth of talar neck is removed in slant fashion leaving behind the conical upper region of talar head and neck. The articular cartilage is denuded continuously leaving behind the original shape of articulating bones (thus there is no reduction in shape and size of foot) a transverse conical trough is created in navicular to accomodate the residual conical talar head.the peroneus brevis tendon is transferred to 2nd or 3rd ray to maintain the normal position of foot. After closing the wound AK POP cast is appilied for 6 wks followed by BK POP cast for another 6 wks. On the whole result has been quite encouraging with only three pseudoarthrosis and negligible shortening in dimensions of foot.
Tendon transfers for residual Erb’s palsy- Our experience.
Prof. A. Devadoss V. Karthi Sundar
Residual Erb’s palsy results in functional limitation of the affected limb due to established contractures with or without the characteristic bony changes. This condition in addition to the physical limitation has an enormous social impact.
Thirty four patients (age 2 to 9 yrs) who underwent tendon transfers for residual Erb’s palsy in our Institute of Orthopedic Research and Accident Surgery from 1987 to 2000 are included in the study. Twenty eight patients were followed up and evaluated. Follow up ranged form 3 years to 13 years (average of 8.5years).
All patients were evaluated for functional outcome using the Modified Mallet Scoring system. Residual deformity, limb length inequality, muscle wasting and also the cosmetic outcome were considered for evaluating the results of the surgical procedure which were good & comparable with the various studies in literature.
Congenital Dislocation Of The Knee
Dr. S. P. Das Dr. P. K. Sahoo Dr. R. N. Mohanty Dr. S. K. Das
Congenital dislocation of the knee was first described by chanssier in 1812 and chatelan in 1822. Incidence is 0.017 per thousand life birds. The deformity may be associated with Larsen. Down’s or Danlos syndrome. The deformity may be part of AGMC. Etiology includes abnormal fetal position, absence of cruciate ligaments and fibrosis of quadriceps. There are two classifications like Levecef Pais and Curtis and Fisher. Repeated manipulation and anterior plaster slab is the method of choice. Failed case needs open reduction. We report management of fourteen knees is nine patients. Four cases were unilateral and five vases were having bilateral involvement. All the cases were classified according to above cited methods. Cases were managed conservatively first. We are able to succeed in three knees with manipulation & slab. Rest eleven knees were undertaken open reduction. We present the method of surgery, problems faced during surgery post-operative complications and results. Most surgically treated knees gain satisfactory range of motion but decreased duadreps strength.
Orthopedic surgery for potentially ambulatory children with cerebral palsy
Dr. Dhiren Ganjwala, Ahmedabad
Introduction: Surgery in patient with diplegia is carried out mainly in ambulatory children with the purpose to improve walking. Author comes across many diplegic children who have potential to walk but because of deformities these children had never walk.
Aim: To study the effect of surgery on potentially ambulatory children with cerebral palsy.
Material: In this retrospective study, 9 children with diplegic cerebral palsy were evaluated. Their walking capacity was 1 – 1 – 1 according to Functional Mobility Scale. However on giving them upright posture with support they were able to make stepping movement. They have reached other milestones of motor development which a child of 10-12 months will achieve (with assistance). These patients underwent multiple (more than 4) surgeries in one sitting.
Result: All except one showed improvement in their FMS at latest follow up at average of 18 months. Two children showed improvement by 1 level for all the three categories while remaining six showed change of two or more levels in all the three categories.
Conclusion: Orthopedic surgery can provide ambulation to non walking children who have potential to walk.
Proximal Fem oral Geom etry in Cerebral Palsy: A Pop ulation -based Cross-section al Study
Abhay Khot Royal Children Hospital Australia
Background/Objectives:
Proximal femoral deformity in the transverse (increased Femoral Neck Anteversion (FNA)) and the coronal planes (increased Neck Shaft Angle (NSA) or “coxa valga”) are common in children with cerebral palsy (CP), contributing to hip instability and ambulation difficulties.The prevalence and significance of these deformities have not been studied in a population-based cohort to our knowledge. Hip instability was examined in these deformities via migration percentage(MP).
Design:
Large population-based, cross-sectional study.
Participants and Setting:
Children with a confirmed diagnosis of CP born within a three-year period were identified from a statewide register with high levels of ascertainment and accuracy. Inclusion criteria: FNA measurement by experienced physical therapists using a reliable, standardized clinical technique (Trochanteric Palpation Test, TPAT), good quality anteroposterior pelvis x-ray and well documented motor type, topographical distribution and GMFCS level.
Methods:
Each child’s unique identifying number was used to obtain clinical (movement disorder, topographical distribution, GMFCS levels, hip rotation range and FNA) and radiological data (NSA and MP) held in either a motion analysis laboratory or hip surveillance database. NSA was measured from an anteroposterior pelvis x-ray with the hips internally rotated by the FNA amount suggested clinically or during fluoroscopic screening of the hip with a guide wire in the centre of the femoral neck. Linear regression analyses were performed for FNA, NSA and MP according to GMFCS.
Results:
292 children were eligible; the results are presented in Table 1. Mean FNA was increased inall GMFCS levels (p (<) 0.001). The lowest measurements were at GMFCS levels I and II; GMFCS levels III, IV, and V were uniformly high (p (<) 0.001). Neck shaft angle was found to increase sequentially from GMFCS levels I to V (p (<) 0.001).
Conclusions/Significance:
This study confirms a very high prevalence of increased FNA in children with CP in all GMFCS levels. In contrast, NSA and MP progressed step-wise with GMFCS level. This information is highly relevant to understanding the origin and management of these deformities. We propose that increased FNA in children with CP represents failure to remodel normal fetal alignment because of delay in ambulation and muscle imbalance across the hip joint. In contrast, coxa valga is an acquired deformity and is largely related to lack of weight bearing and functional ambulation. The high prevalence of both deformities at GMFCS levels IV and V explain the high rate of displacement in these hips and the need for proximal femoral realignment surgery in the prevention and management of hip displacement.
Septic Arthritis in children: An comparison of culture negative and culture positive cases
Menon J, Patro DK.
Department of Orthopedics, Jawaharlal Institute of Postgraduate Medical Education and Research
(JIPMER), Pondicherry - 605006.
E-mail address of the presenter:Jag4ishmenqayahc.ck
Identification of offending organism in septic arthritis not only confirms the diagnosis but also provides guidelines for therapy. However, rates for positive culture are variable. The natural history, clinical presentation, laboratory profile and the outcome of patients with identifiable pathogen and those without are said to be different. We compared cases of septic arthritis with a positive culture with cases where no organism could be grown, in an attempt to identify the differences between these two groups. Ninety seven patients with septic arthritis were identified in the three year period of Jan 2002 to Dec 2004. Culture postivity was 37.83%. Demographic data, clinical and laboratory data were analyzed to assess the difference between culture negative (n= 58) and culture positive (n= 39) groups. Staph aureus was the most common isolate with 44% strains being methicillin resistant. No significant difference was noted in any of the clinical or laboratory findings except delay in presentation (11.1 ÷1- 8.6 days vs 5.4 +1- 4.1 days). History of prior treatment, radiographic changes was more pronounced in the culture negative group Septic arthritis is a disease with high morbidity and the absence of an identifiable pathogen does not appear due to influence the clinical profile of the patient or the natural history of the disease.
REVISION SURGERIES FOR FAILED SURGICAL REDUCTION IN DEVELOPMENTAL HIP DYSPLASIA
PRESENTING AUTHOR – Dr. Arjun A. Dhawale
CO - AUTHOR- Dr. Ashok N. Johari
E-mail - arjundhawale@hotmail.com
Phone no - 022-24365050
KEY WORDS - Revision surgeries, failed surgical reduction, DDH
AIMS - To study the causes of primary failed surgical reduction and discuss the surgical options, results and complications of revision surgery.
MATERIALS AND METHODS –
29 patients (30 hips) underwent revision surgeries for failed open reduction in DDH. Complete follow-up records (mean follow-up since revision surgery - 4.4 years) are available in 16 patients (19 hips). In 6 cases, open reduction was done and in 13 cases, open reduction was combined with supplementary acetabular / femoral procedures. Clinical and radiological details before revision surgery and at last follow-up were recorded. These included Severin grading, Acetabular index, CE angle, lateral subluxation, shape and size of head. CT and MRI films were reviewed. The indications for surgery were redislocation, subluxation or residual acetabular dysplasia. Surgical details were recorded. Results were graded with the Ponseti score, Severin grading and Seddon and Trevor clinico-radiological score. The incidence of complications and AVN were recorded.
RESULTS AND DISCUSSION –
The preoperative Severin score was 3 or above in all cases. At revision surgery, operative findings included adhesions and soft tissue obstructing reduction, head changes, increased anteversion and acetabular factors. Open reduction was done in 10, supplementary femoral procedures in 12, and acetabular procedures in 18 cases. Results - Ponseti score of 1 or 2 in 9 cases, Severin score of 1 or 2 in 8 cases, Seddon Trevor grading - excellent in 4 and good in 6 cases.
CONCLUSIONS –
Improperly performed primary open reduction leads to failure of primary open reduction. The revision surgery requires adequate pre-operative planning, meticulously performed open reduction and a combination of acetabular and femoral procedures.
SHAHS MODIFIED FUNCTIONAL MOBILITY SCALE - THE HAND GRIP MODEL FOR DEVELOPING COUNTRIES
DR VIPUL SHAH MS ORTHO*, MANSI AGARWAL BPT*, DR ASHOK JOHARI € MS ORTHO,DR VIRAJ SHINGADE ₤ MS ORTHO,SUNIL SINGH BPT**,MD.ALIM BPT*HIMANSHU SINGH DPOE**
The function of cerebral palsy patients is governed by their inherent energy generation potential along with their coordination and higher functions .A number of methods including oxygen usage, gait labs with dynamic gait analysis are used to assess this functional potential .Third world countries with paucity of funds and with absence of sophisticated know how are at a disadvantage and hence PRS and physiological cost index are worthy parameters to gauge walking potential. The functional mobility scale is a handy tool to assess the childs walking energy costs In third countries in general and India in particular the absence of barrier free environment and coupled with the social stigma attached to the use of walking aids makes the parents resort to forcing the child to use hand support instead of walking aids hence the need to modify FMS was felt . The scale is based on FMS and yet inherently different and suited to these needs. The scale also takes into account in addition to walking potential grossly, the time of stops and the number of stops which indirectly reflects dynamics of energy consumption
Modified Functional Mobility Scale –
- independent on all surfaces and on curbs, flight of 10 stairs.
- Independent on level surfaces, curbs, flight of 10 stairs.
- Uses single hand support:
- Holds with light feathered touch without much pressure being exerted.
- Grips with single hand onto the finger.
- Mother’s hand is held by the child
- Mothers forearm is gripped by the child
- Mother holds the child’s hand.
- Mother /attendant grips the child’s arm/forearm
- Double handed support:
- Independent 3a/ uses a single crutch/3a/b/c/d/e/f
- 3b/ uses a single crutch/3a/b/c/d/e/f
- 3c/ uses a single crutch./3a/b/c/d/e/f
- 3d/ uses a single crutch./3a/b/c/d/e/f
- 3e/ uses a single crutch./3a/b/c/d/e/f
- 3f/ uses a single crutch./3a/b/c/d/e/f
- Bilateral crutch.
- Holds parents arm with both hands
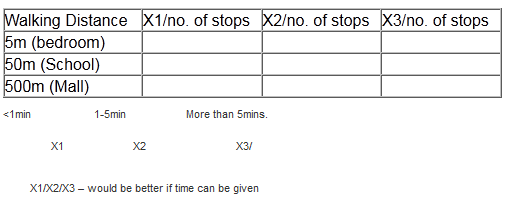
TOTAL DISTANCE TRAVELLED WITH COMBINATION OF SINGLE HAND/DOUBLE HAND SUPPORT
6. Asks the parents to lift him /her.
The main characteristics which define any evaluation method are1)repeatability2) distinction between different classes3)low inter and intra observer variability
Additional qualities required out of a scale in developing countries are
- cost effectiveness and reliability on basic equipments
- admissibility by less trained staff
We have measured the different classes with physiological cost index repeatedly and found that the different classes are inherently different from one another not only in terms of support required but also in terms of the PCI as wheel chairs are sparsely used due to absence of barrier free environment
ARIHRODIASTASIS OF HIP JOINT IN PERTHES DISEASE
Dr BIPN A GANGURDE (AUTHOR)
DR G.S.KULKARNI
DR RUTA.M.KULKARNI
KEY - Perthes disease.Articulated hip distractor
INTRODUCTION - Late onset perthes disease have a bad prognosis.There is stiffness of the hip joint .Hip distraction by an articulated distractor has improved the prognosis of such patients
MATERIALS AND METHODS - In our hospital at Swasthiyog Prathisthan Miraj 8 cases were studied out of which 3 males and 5 females.Age 10 to 13.5 yrs.Al1 had stiffness. Articulated hip distractor was applied to all .Distraction was done till shentons line was corrected. 2 pins in the supraacetabuar region, 2 in the iliac crest 3 pins in femur and hinge 8 mm proximal to the centre of head of femur. RESULTS: Pintract infections were minor complications .Pain of the patients was decreased and rom of the patients improved.
CONCLUSION - Unloading the femoral head and restoration of the joint space impru ed function of the patients.
Closed nailing for paediatric forearm bone fractures - Is it always closed?
Dr. Ashutosh Bhosale Dr. M. Rajeev Rao. Dr. M. Ramesh, Dr. Manjunath, Dr. Yogishwar
Institution - Jubilee Mission Medical College and Research Institute, Thrissur, Kerala, India
Introduction -
Paediatric Forearm bone fractures are commonly treated by orthopedic surgeons. Current literature unequivocally supports nailing for stabilization of them to prevent malunion and delayed union. In this miniinvasive interventional era, surgeon is always compelled to do closed nailing. But is it always closed? & At what cost?
Materials
We retrospectively reviewed forearm bone fractures in children managed at our institute between 2004 and 2005. There were 96 cases of diaphyseal radius and ulna fractures. All were managed with intramedullary square nailing. Two groups were made viz. Gr A Successful closed nailing in 1 or 2 attempts. Gr B closed nailing requiring> 5 attempts and which required open reduction.
Results
Gr A had 72.9%(70/96) cases while Gr B had 27.08%(26/96) cases which required open reduction for passing nails across the fracture site. The average surgery time for gr A was 20 minutes while in gr B required average 45 minutes and the difference was statistically significant with p value < 0.05. There was no difference in union rate and time in both groups. In gr B due to more postoperative edema, the hospital stay was average 5 days while in gr A it was only 2 days. It also increased total cost of treatment. Open reduction was required due to preoperative edema, late presentation or late surgery, soft tissue interposition, overriding or due to false tracks. Open reduction was required more in radius fractures.
Conclusion
Closed nailing in forearm bone fractures is not always possible. After 1 or 2 attempts at closed nailing, open reduction should be done to avoid soft tissue insult. As the union rate is same, aim should be minimal surgery time and soft tissue damage whether closed or open.
Prediction of Complications of Limb Lengthening in Children
PN Gupta,
Department of Orthopedics,
Govt. Medical College Hospital,
Chandigarh.
Limb lengthening using distraction osteogenesis with external fixators has revolutionized the management of segmental bone defects. However limb lengthening is often marred by complications which may be more severe than the original condition itself. This is especially true in large lengthenings. We conducted a study in 20 lengthenings of bone in children with an average age of 4 years and 4 months, where lengthening of the bone was done by an average of 30% of the original length of the bone. The complications were grouped as benign, serious, requiring re-surgery, and severe requiring abandoning of the lengthening program. Eight additional procedures under general anesthesia were required during lengthening process and all these procedures were required in patients lengthened more than 20% of the original length of the bone. However the most severe complications were seen in congenitally short limbs, requiring premature abandoning of the lengthening program. We recommend that large lengthenings in congenitally short limbs should be done with caution and those congenitally limbs requiring more than 20% lengthening should be done as staged procedure. In all other conditions, large lengthenings more than 20% is possible without abandoning the lengthening procedure and severe complications, but may require additional procedures under general anesthesia.
ARTICULATED HIP DISTRACTION
CONSERVATIVE SURGERY FOR ARTHRITIS IN YOUNG PATIENTS
DR. SANDIP VYAS, M.S. (ORTH.), DNB (ORTH.), ILIZAROV FELLOW (USA)
DR. PREMAL NAIK, M.S. (ORTH.), DNB (ORTH.)
DR. ASHOK N. JOHARI, M.S. (ORTH.), DNB (ORTH.), MNAMS (ORTH.), McH
(LIVERPOOL)
Between 1993 and 2007, patients with a variety of hip diseases were treated with articulated distraction of hip. The patients ranged from 7 to 18 years of age (mean 12.5 years). The primary diagnoses included malunited acetabular fractures with chondrolysis in two patients, dislocated head with AVN in SCFE with chondrolysis, stiff hip following DDH surgery, septic chondrolysis, idiopathic chondrolysis and three patients with perthes disease. A standard dynamic axial fixator with a single axis articulating unit was used to create a 5 mm joint space. The Fixator allowed flexion and extension motion and remained in place for 8 to 10 weeks. Six hips were treated by the Dynamic Axial Fixator (Orthofix Fixator) and three hips were treated by Ilizarov Apparatus. The follow up period ranged from two to nine years. Assessment was performed by clinical and radiographic review using the Harris Hip Score. The results were good in seven hips and fair result in two hips.
Congenital Scoliosis – our experience
Dr Ramani Narasimhan
Sr Consultant Pediatric Orthopaedic Surgeon
Indraprastha Apollo Hospitals
New Delhi
E-mail: ramanirn@hotmail.com
We share our experience in dealing with 16 cases of congenital scoliosis with varied presentation and analyze our management in terms of available case studies in literature. These patients comprised of 11 boys and 5 girls ranging from 1 month of age to 8 years of age, who attended clinic at Indraprastha Apollo Hospitals, New Delhi, between June 2002 and December 2006. Apart from the x-rays of the spine, all patients underwent MRI of the entire spinal axes with scout films of brain, ultrasonography of abdomen and pelvis, and cardiac assessment. All cases were assessed clinically & radiologically at 4 month intervals to assess for any progression. Fourteen curves demonstrated significant progression and required appropriate surgical management according to the cause and site of the curve, and age of the patient. Follow-up ranges from 1 year to 4 years. Natural history of these congenital curves needs to be thoroughly understood before embarking on their treatment. Anticipating & predicting outcome remains the key. A multidisciplinary approach towards their management is the best bet for achieving success.
PAEDIATRIC CERVICAL TRAUMA – PATTERNS OF INJURY AND MANAGEMENT
Dr Arvind G Kulkarni, Bombay Hospital, Mumbai
Dr Andrew Cree, Royal Alexandria Hospital, Westmead, Sydney, Australia
INTRODUCTION : Paediatric cervical trauma is relatively rare and few reports exist regarding the injury profile , especially the use and efficacy of modern instrumentation in children. The aim of this study was to review the management of paediatric cervical trauma at a major teaching hospital.
METHODS : The clinical charts and imaging studies of children with cervical spine injuries managed between January 2000 and July 2006 at a tertiary children’s hospital were retrospectively analysed for patient demographics, mode of injury, neurological status and management. Complications and the use of implants was evaluated.
RESULTS : 33 cases had structural injury needing bracing or surgical intervention, the ages of the patients ranging from 1year – 15 years (average – 8.7 years). There were 21 males and 12 females. Motor vehicle accidents (15), sports injury (12) and domestic injury (6) were the causes of injury. . A total of 12 patients (36.4 %) were managed operatively, 5 patients (15 %) died as a result of trauma and the rest (16 cases, 48.5 %)) were treated conservatively. There were 14 (42.5 %) upper cervical injuries (C0-C3), 14 (42.5 %) lower cervical injuries (C4-T2), 4 cases (12 %) involving both upper and lower cervical levels and one case of anterior spinal cord infarct (3 %). A total of 9 patients were victims of polytrauma. Modern spinal titanium instrumentation utilising locking screws, cables was employed in patients needing operative stabilization. There were no complications and no cases of implant failure. Spinal cord monitoring was utilized wherever possible, but the safety of motor evoked potentials has not been validated in children less than four years of age, and they were frequently unreliable in the multi-trauma situation, especially in the presence of a concomitant head injury.
DISCUSSION : Cervical trauma although rare, is the commonest region involved in paediatric spinal injuries. Motor vehicle accidents form the commonest cause of cervical injuries. Pre-operative CT scans and MRI are critical for accurate diagnosis and meticulous planning. Proximal cervical trauma, especially atlanto-occipital dissociation can be a challenging diagnosis, but modern instrumentation can be utilized successfully. Although the cases are limited, preliminary experience shows that rigid internal fixation with modern instrumentation is safe and effective in paediatric cervical trauma for all age-groups. Customisation of routine inventory as well as adaptation of miniature instrumentation systems utilized in other fields of orthopaedics (eg. phalangeal plates) is necessary for successful instrumentation in the paediatric cervical spine. Development of specialized paediatric cervical instrumentation is a prospective area of further research.
A Novel Approach to Management of Idiopathic Scoliosis
Amit Bhanti
Management of idiopathic-scoliosis has always been a topic of controversy. There have always been differences in opinion amongst care giving professionals on what’s the best approach. There is enough data to support that both surgical as well as conservative approaches work well, depending on type of curve, magnitude, age, skeletal maturity and many other factors.
This paper deals with a fast developing conservative approach of CAD/CAM assisted management of scoliosis. The use of CAD-CAM technology in the treatment of adolescent idiopathic scoliosis was first reported in Spine in 2005 by a team of French physicians and researchers. This was quickly followed the same year by the preliminary outcomes of a second medical team in China. The following is an introduction to a third CAD- CAM assisted approach developed by Dr. Miguel Gomez, of Bogotá Colombia, now a practicing Orthotist in Houston, TX, USA. This approach has been adopted for majority of our scoliosis patients that we treat in central Illinois, and have been assisting Miguel Gomes in further development of the system.
The presentation will outline the whole process, from evaluation of patients to fitting of the finished Orthosis. A patient case study will elaborate on the results and efficacy of this technique.
OUTCOMES OF OPEN REDUCTION AND INTERNAL FIXATION FOR FRACTURE OF LATERAL HUMERAL CONDYLE IN CHILDREN
Dr. Chirag Bhalvani; Dr. Paresh Golwala
Fractures of lateral humeral condyle constitute 16.9% of all distal humeral fractures in children. It is an intra-articular injury and, if not treated accurately, can damage the elbow joint. In spite of accurate open reduction and fixation, it is usually found to have many complications. This study was undertaken to study the outcomes of open reduction and internal fixation in management of close fracture of Lateral Humeral Condyle in Children. Twenty five children (between the age 4 to 11 years) having fracture of lateral humeral condyle, who were treated by open reduction and internal fixation were studied and followed clinically and radiologically over an average period of 2 years. The average age of patients was 7.7 years with involvement of left side in 19(76%) patients. Out of 25 patients, 2 patients developed non-union of which, 1 was due to post operative infection. Fish-tail deformity was observed in 8(32%) patients; while premature epiphyseal fusion was found in 10(40%) patients. 22(88%) patients had a change in the carrying angle (average 4.3o), which was functionally and cosmetically insignificant. An interesting finding of Radial head enlargement with hastened ossification of its epiphysis was observed in 15(60%) cases. The average increase in radial head size radiologically was 1.4mm and it was not associated with decrease in elbow range of movement. Postero-lateral spur formation was found clinically in 23(92%) cases. Another noteworthy finding observed in all the patients having postero-lateral spur formation was an increased condylar width radiologically and clinically, with an average increase of 3.6mm. Apart from routine complications, Radial head enlargement noted in 60% of the patients has no mention in the literature so far. Also, the postero-lateral spur observed was associated with increase in the condylar width radiologically and clinically. These two findings may be interrelated to each other, specially the former to the latter. Key words: Fracture of lateral humeral condyle in children, radial head enlargement at follow up, postero-lateral spur, increased condylar width.
Ender Nailing An Economical Boon For Paediatric Femoral Diaphyseal Fractures.
Author: Manj unatha.K.R.
Co authors: M. Rajeev rao, Ramesh. M.
Introduction : Paediatric diaphyseal femoral fractures account for approximately 1.6% of all fractures seen in this population. Flexible intramedullary nailing has been the proven forerunner among treatment options for these fractures. Heinrich et al popularized Ender nailing which paved the way for recent trend of global use of titanium elastic nails. But in this part of subcontinent a nail functionally equivalent to titanium elastic nail at a lower cost is desirable.
Purpose : To evaluate the clinical, radiological and functional outcomes of Ender nailing in paediatric femoral diaphyseal fractures and comparison of the same with outcome of titanium elastic nails.
Materials and methods : 26 consecutive children with femoral diaphyseal fractures treated with Ender nailing were evaluated prospectively. The average ages of male and female patients were 10.2 and 10.5 years with standard deviations of 2.6 and 0.5 respectively. .In 20 patients retrograde nailing was done with 2 nails. In 6 patients one antegrade and one retrograde nailing was done. .Average duration of surgery was 22 minutes with standard deviation of 4.5. All patients were mobilized and allowed partial weight- bearing in a functional brace in the early postoperative period. Among the associated injuries head injury was the significant one occurring in 4 patients followed by abdominal injury in 2 patients. Average hospital stay was 7 days with standard deviation of 2.81. Average followup was 18 months. Evaluation was done with Flynn’s criteria and AAOS paediatric functional outcome score version 2. We compared our results with titanium elastic nailing studies of Ligier et al and Flynn et al
Results : In our study oblique,spiral and transverse types are seen in the ratio of 2; 1 ;2. All the fractures united between 6 to 8 weeks time. Only one patient had limb lengthening of 1.2 cm. 4 patients had knee stiffness.3 patients had coronal angulation and 4 sagittal angulation within acceptable limits.20 were graded excellent,5 good andi poor by Flynn’s criteria. Our results were comparable to that of Ligier et al and Flynn et al
Conclusion : In our experience, Ender nailing highly effective for the treatment of children 6 to 14 years old with femur fractures and outcome equal to that of titanium elastic nailing at a lower economy can be achieved.
Intramedullary stabilization of ulna in Monteggia fractures – Is it sufficient?
Dr. M. Ramesh Dr.M.Rajeev Rao, , Dr. Manjunath, Dr.Bhosale Ashutosh,Dr. Yogishwar.
Institute Jubilee Mission Medical Collage Hospital, Thrissur, Kerala, India-680 005
Introduction : A watchful eye is required to diagnose Monteggia injury in children. The bowing of ulna is the most important clue for the identification of the lesion. It is must to correct bowing or alignment of ulna to get radial head in place. It is preferred to stabilize the ulna by intramedullary implant.
Materials and methods : In our institute, 106 cases of monteggia fracture dislocation were treated during 1996 to 2006. The age range was between 4 years to 15 years. There were 80 with anterior type, 12 with posterior while 14 had lateral type. All the fractures were managed intramedullary implants like K wires, ulna nail or screw fixation. The closed reduction was possible in 94 cases while 12 required open reduction for ulna. In all cases radial head was easily reduced after ulnar stabilization except in 2 cases which required open reduction of radial head.
Results : All the cases were fixed by intramedullary devices for ulna fractures and reduction of radial head was possible. The average operative time was 20 minutes with SD 3 minutes. The blood loss was minimal of up to 10 cc. The average flexion was up to 110°. There was no case with growth arrest or limb length discrepancy. Full functional recovery was possible. The removal of implant was easy but pin breakage and migration of wire was seen in 5 cases. Olecranon bursitis was seen in 12 patients which resolved after nail removal.
Conclusion : Intarmedullary fixation is an easy, fast method for ulna fracture which allows closed reduction of radial head. As it is minimal invasive with minimal blood loss, it is preferred method for monteggia fracture management.
-
POSTER ABSTRACTS
Unusual presentation of Back ache - A case report
In this era of fast life, fast food, fast food, fast game, we tend to overlook the vague presentation of back ache among school going children, occurring to the prevalence of school bag syndrome, malingering etc., We share our experience of a young boy who presented with an unusual back ache of 2 years duration. Master A, 14 years, presented to us with a history of long standing back ache of 2 years duration, treated at many hospitals in and around. The pain was insidious to start with progressive, aggravated on activities. X — rays of pelvis revealed scleorosis at the sacroiliac joints. Chest expansion was diminished, schoebers test was positive. HLA B27 was done, which became positive. He was diagnosed to have a “Juvenile Onset Ankylosing Spondylitis”, was treated symptomatically with analgesics, active chest physio was started and patient educated. Juvenile Ankylosing Spondylitis is a rare disorder. The onset is usually at 12 — 14 years and progresses. In our daily meeting of children as out — patients, the probability of us missing children with significant problems is high. Hence the vague complaints of back ache in school going children should not be overlooked.
Two stage limb lengthening in Ollier’s Disease
Author: Dr. G. Mukesh Mohan, M.S, DNB Ortho
Asst. Professor of Orthopaedics,
KAPV Govt. Medical College, Trichy.
ABSTRACT
Oilier’ s Disease or Multiple enchondromatosis is a rare disorder causing multiple bony deformities. IN long bones, it causes angular deformities and limb length discrepancy especially unilaterally. One such patient a 12 year old girl presented to our department with equines deformity. On examination she had true shortening of right femur and tibia of 5 cm and 6 cm respectively. She had genu varum of right knee. Skeletal survey showed multiple cartilaginous lesions in proximal femur, distal femur, proximal tibia, distal tibia and right ilium. Two stage limb lengthening was planned for this patient. In the first stage, tibia! lengthening was achieved using Ilizarov fixator with foot assembly. Then after removal of Ilizarov fixator, femoral lengthening was achieved using Limb reconstruction system fixator. During the period of lengthening, no complications except for minimal procurvatum deformity of proximal tibia was encountered. At the end of 5 months, she has gained limb length equality.
CONCLUSION
Two stage lengthening of femoral and tibial shortening was easier and safe in gross shortening.
Posterior dislocation of elbow with ipsilateral distal radius and ulna fracture in a child – A case report
S.Saseendar, D.K.Patro, J.Menon, Satyanarayanan
We report a rare case of closed posterior dislocation of elbow with ipsilateral Gustilo Anderson type II compound fracture radius and ulna distal one-third in a 11 year old boy who had a fall from height. There was no neurovascular deficit at presentation. The elbow dislocation was treated with closed reduction and the forearm fracture with debridement, open reduction and Kirshner wire fixation. The patient was discharged on a long-arm cast. The mechanism of injury leading to the rare association of elbow dislocation with ipsilateral distal both bone fracture and the outcome of treatment is discussed.
BACK PAIN IN A 15 YEAR OLD BOY - A CASE REPORT
We describe a case of back pain in a 1 5yr old boy which turned to be the visible part of a massive iceberg. This boy presented with hlo back pain for 2 months which started after lifting a heavy weight. He also gave h/o on & off fever for past 4 months. He was receiving native treatment and had also visited couple of centers before reaching us. General examination showed a malnourished kid with pallor. Local examination of spine showed diffuse tenderness over lumbar and lower thoracic spine with paraspinal muscle spasm. His basic investigations showed anemia, leucopenia, neutropenia and an elevated ESR. Diffuse osteoporosis was present in radiological survey. Subsequently bone marrow study was done which revealed marrow infiltration with round cells — suggestive of Acute Lymphocytic Leukemia. Further immunocytochemical studies were done. Patient underwent chemotherapy for one month but inspite of treatment his life could not be saved. The incidence of back pain in children is only 30% in comparison to adults. The review of literature also shows that any child presenting with back pain should be taken seriously and investigated to diagnose the cause.
Key words: Adolescent back pain, Leukemia
CLOSED TECHNIQUE OF TREATMENT OF PAEDIATRIC DIAPHYSEAL FOREARM FRACTURES WITH INTRAMEDULLARY NAILING
Dr. Jerry Jacob Manjuran. Dr. G.S. Kulkarni, Dr. Vidisha S. Kulkarni., Dr. Ruta M. Kulkarni
Key:
Closed. paediatric diaphvseal forearm fractures. nailing, square nail, management.
Aims:
- Results of intramedullarv nailing.
- Duration of surgery.
- Postoperative function.
- Chances of Infection.
Materials and methods:
Anal sis of 50 cases of paediatric diaphyseal forearm fractures were done in ages from 9 to 13 yrs. All of which were treated with closed reduction and internal fixation with intramedullary nailing.
Discussion:
Diaphyseal fractures of forearm is very common in children. Even moderately displaced fractures were treated with closed reduction and internal fixation with intramedullarv nailing.
Conclusion:
Results were graded into excellent. good. fair and poor. Results were excellent in 45 cases. good in 5. There were no poor cases. Closed reduction and internal fixation with intramedullarv nailing proved to be an effective treatment as children have high remodelling potential. The chances of infection have diminished. The time consumed during surgery was reduced. Post operative function of the limb is retained to normalcy.
Paediatric Finger tip injuries – management
Dr. B.Suresh Gandhi, Dr.Mohammad thahir, Dr.Sanddep saxena .Dr. Ravi Kumar.
Department of Orthopaedics Southern Railway Hospital, Perambur Chennai 23
Background: Injuries of the fingertip are common among children. Outcome depends on initial evaluation and management. Parents need to be educated about preventive measures
Objectives: To evaluate the mode of injury and various modalities of management of fingertip injuries among children.
Study design: A retrospective study of finger tip injuries that presented to our emergency department and which were treated using a defined protocol.
Subjects: 13 children with finger tip injuries presented to our emergency department during the period from Jan 2006 to May 2007. The patients ranged in age from 2 years to 12 years. Most of the children had history of door crush injury. The techniques used were primary closure, terminalisation, , composite grafting and dressings alone.
Outcome measures: The outcome of the treatment protocol was assessed by healing of the wound, function of the hand, and the period of time taken to return to normal activities.
Results: 95 % of the patients were achieved primary wound healing at end of 2 weeks.
Conclusion: Meticulous initial evaluation and a clear management protocol in treating finger tip injuries results ingood hand function
Sliding — angulation osteotomy of proximal ulna for persistent radial head dislocation: A novel technique
Dr. K Venkatadass
Dr. S. Rajasekaran
Dr. Ajoy Prasad Shetty
Abstract:
Radial head dislocation in a Monteggia lesion is often missed in children during the initial presentation and they present later with persistent radial head dislocation and associated malunited ulnar fracture. This is a complex problem where the child has got restriction of movement, deformity and also instability. A variety of intra-articular, extra- articular and combined procedures have been described from many centers with variable results. We herein describe a novel technique of sliding angulation osteotomy of the proximal ulna to achieve a stable reduction of the radial head. In this a sagitally oriented ‘z, shaped osteotomy of the ulna was done at the plastic deformity site which was slided and angulated till a stable reduction of the radial head was achieved. The procedure is completely extra-articular and the technique is relatively simple with good clinical end- result. This single stage procedure addresses the deformity, dislocation and decreased range ofmotion and hence serves as a simple solution for this complex problem.
Keywords: dislocation, radial head, chronic, ulnar osteotomy
Talwalkar’s Square nails -A cost effective, Closed nailing for forearm fractures in children
Author — Dr. Yogishwar AN.
Co-authors - Dr. M. Rajeev Rao, Dr. M. Ramesh ,Dr. Manish Chacko, Dr. Manjunath
Institution — Jubilee Mission Medical College and Research Institute, Thrissur, Kerala, India
Introduction:
Conservative treatment of forearm fractures is frought with complications of cast, compartment syndrome. The malunion and bayonet apposition are synonymous with cast application and directly affect functional recovery. Prolonged hospitalization and high cost associated with plate fixation makes choice of treatment difficult, We prospectively evaluated outcome and cost effectiveness of closed nailing of forearm bone fractures in search of a better treatment
Materials and methods:
22 children between age group of 5 to 15 yrs with forearm fractures were prospectively treated with closed intramedullary nailing with Talwalkar’s Square nails between January 2005 to December 2007. Diaphyseal fractures of both bones forearm were nailed with flexible square nails and were given splints for 4 weeks. Patients underwent implant removal once there was clinical and radiological union of fractures.
Results:
All fracture united by 6 to 8 weeks. Average follow up was 50 weeks, with average age group of over 8years. Clinical functional outcome according to Price criteria were 15 patients excellent, 5 good and 2 fair. There was no limb length disparity, Forearm rotations was equal to opposite side in 80 % cases. Radiologically average angulation of radius and ulna was < 5 degree at last follow-up. There was no case with bayonet apposition, malunion, re fractures of bones. Average surgery time was 20 minutes ±10 minutes without any blood loss. The only complication noticed was of infected olecranon bursitis which resolved after implant removal in 2 patients. None of our forearm fractures had compartment syndrome.
Conclusion:
Intramedullary Square nail fixation is an easy and fast method for forearm fractures with minimal blood loss and minimal scar. It prevents malunion and bayonet opposition. Full range of movements was achieved without any significant complication. As cost of implant is very less and hospital stay is reduced to average of 2 days closed nailing for radius and ulna fracture is a effective way to reduce treatment cost and hospital occupancy burden.
Ultrasound: The third eye of paediatric orthopaedic surgeon
Dr. Premal Naik
Associate Professor of Orthopaedics, N H L Municipal Medical College , Ahmedabad
Key words: ultrasound, DDH, osteomyelitis, septic arthritis
Introduction: For many years radiography has become an integral part of orthopaedic examinations. All orthopaedic surgeons depend heavily on radiography to make final diagnosis in most of the conditions. Unfortunately radiography has the disadvantage of being able to depict only bone and in children only the ossified portion of the skeleton. This makes it less important for diagnosing various conditions in children and in soft tissue problems. MRI has become gold standard in diagnosing soft tissue problems, but limited availability and cost prohibit its use as routine investigation. In such circumstances ultrasound provides useful information in many paediatric orthopaedic problems.
Material and Methods: We have been using ultrasound in paediatric patients since 2001. We present our series of patients from 2002 – 2006. Ultrasound was used very effectively to diagnose DDH (12 pts), PFFD (3), osteomyeltis(7), septic arthritis of hip(18), knee(3), ankle(1), elbow (1) and shoulder(2) and soft tissue abscess(3). It was also very useful in patients with congenital knee dislocations (13) and AMC (1).
Results: Ultrasound was found very accurate in diagnosing hip dysplasia in patients with suspicion, AMC and congenital knee dislocations even when X ray was normal. It is very useful in identifying presence of capital femoral epiphysis in patients with PFFD. It is very handy in diagnosing periosteal elevation, subperioesteal abscess and epiphyseal involvement in patients with Osteomyelitis. It is only useful investigation for septic arthritis mainly of hip joint in patients less than 3 months in age where it shows fluid collection and displacement of femoral head which is not visible on x ray.
Conclusion: Ultrasound is a very useful and handy tool for diagnosing many paediatric orthopaedic conditions. It is very useful in diagnosing and monitoring neonates with DDH. In paediatric musculoskeletal infections it can provide diagnosis and obviate the need of MRI which is very expensive and needs anesthesia in small children. Easy availability, low cost and no radiation hazards make it ideal investigation in many paediatric disorders.
THE USE OF IRRADIATED ALLOGRAFT IN A PAEDIATRIC POPULATION:AN INDIAN EXPERIENCE
V. Shingade, A. Johari, V. Shah, A. Lobo Gajiwala, C. D’Lima
Contributing Institutes:
Children Orthopaedic Care Institute, Daya Chambers, Ajni square, Wardha road, Nagpur.
Children Orthopaedic Centre, Boby Apartment, Lady Jamshedji Road, Mahim West, Mumbai, India.
Tissue Bank, Tata Memorial Hospital, Parel, Mumbai, India.
Abstract:
Lyophilized, irradiated bone allografts available for the first time in the country from the Tata Memorial Hospital Tissue Bank were used in 30 paediatric patients from January 2001 to August 2004. They included 20 patients of scoliosis of various origin and 10 with assorted orthopaedic conditions including 1 congenital kyphosis, 2 Pott’s spine, 1 Perthes disease, 1 developmental dysplasia of the hip (DDH), 1 fibrous dysplasia and 4 with bone defects either due to trauma, a cyst or removal of hardware. Morsellised allograft was used in 28 patients. In those cases of scoliosis in which ribs were resected out during costectomy, the morsellised allograft was mixed with morsellised rib autograft. Non –morsellised femoral head grafts were used in 2 patients, one a case of varus open derotation osteotomy in Perthes disease and the other an acetabuloplasty in DDH. Patients were followed at intervals of 8-12 weeks and radiological evaluation was done periodically. The follow up period ranged from 1 year to four years post surgery. All patients with scoliosis showed excellent union at the grafting site with non progression of curve and no signs of loosening at implant site. The two patients, in whom non morsellised femoral head grafts were used, both showed incorporation of the graft with good fusion within a four month period. None of the patient had infection, non-union, pseudoarthrosis, fracture at the graft site, or any other complication.
Key words: Lyophilised irradiated allograft, orthopaedic deformities, paediatric population.
Palliative Care in Paediatric Bone Tumors
Karthik S Murugappan, S Alam Khan, S.Rastogi, *S Bakhshi
Dept. of Orthopaedics, *Dept. of Medical Oncology
All India Institute of Medical Sciences, New Delhi
Introduction:
Malignant bone tumors in children constitute 6% of total pediatric tumor load. Incidence of malignant bone tumors is particularly high in developing countries where most of these patients present at a late stage when curative therapy is not possible. Palliative care to pediatric tumor patients is the most needed but least cared for issue.
Materials and Methods:
We retrospectively evaluated the symptoms in a group of 139 children with malignant bone tumors over a period of 10 years. Of these 38 children had presented as end stage disease with systemic metastasis. Pain was the predominant symptom besides problems due to immobility and wound complications. Children were divided in three groups based on the type of treatment given for pain. Group I had patients who underwent palliative amputation, Group II had kids who underwent palliative radiotherapy and Group III children were managed by drugs alone. Pediatric Visual Analog Scale was recorded in all 38 kids prior to and after treatment.
Results:
Osteosarcoma and Ewing’s sarcoma predominated the diagnosis in these children. Group I had 12 children, Group II 18 and Group III had 8 patients. The Pediatric Visual Analog Scale recorded on treatment completion showed that the best results in pain control were obtained with amputation.
Discussion:
Children suffering from bone tumors have significant symptoms to be addressed even when a curative treatment program is planned and hence a palliative physician is an essential part of the treating team. Proper assessment and treatment of pain is essential. Good nursing care and early mobilization will prevent debilitating complications of immobility. Amputation seems to offer the best mode of pain control in patients with end stage cancer of the extremity. Proper sensitization of the parents is necessary before taking the decision. In our study, phantom limb sensations and pain were noted in none of the children who underwent amputation. Patients who were not amenable to amputation were put on radiotherapy and drugs according to the histological type of tumor. Our study has the limitations of a small number, non consideration of other symptoms for evaluation and lack of comparability with regards to the site of tumor. Larger well structured studies are needed to bring out the scope of palliative care in pediatric bone tumors.
Conclusions:
Children with bone tumors form an important subset of patients in need of palliative care. A team approach is necessary in treating a child with the diagnosis and always, it is a continuum of care of the child and the family. Pain is the predominant symptom in end stage patients and amputation seems to offer the best pain relief. Issues about communication to the child have to be addressed. Larger studies are necessary to evaluate the care of children with bone cancers.
SOFIELDS PROCEDURE - OUR EXPERIENCE
Correction of limb deformities in Osteogenesis Imperfecta has always been a challenging task to any Orthopaedic Surgeon. Sofield multiple osteotimies, Realignment and TM nailing is the most widely used procedure for deformity correction. We present our experience with this procedure. 4 patients in the age group of 4 — 7 were chosen for this procedure. Rush nails were used in all cases after the Osteotomies. All 4 underwent procedures in femur and tibia. Of this, 1 patient had the procedure done in the humerus also. 1 patient developed protrusion of nail in the knee joint after femoral nailing, which required a secondary procedure. All our patients had adequate callus by 4 — 5 weeks post surgery and had an uneventful union. Even though the results are gratifying, the patient needs careflil monitoring and long term prognosis may be guarded.
-
Medal Paper session
Use ofPonseti’s technique in recurrent clubfeet following Kite’s method of correction.
Dr. K Venkatadass Dr. S. Rajasekaran Dr. Ajoy Prasad Shetty
Abstract:
We report the results of eighteen recurrent clubfeet in thirteen children following Kite’s method of casting treated successfully by Ponseti’s technique. The average age was 8.3 months. The average preoperative Pirani’s midfoot contracture score was 1 .8; hind foot contracture score was 2.4; and total score was 4.2. All patients had full correction of deformities with plantigrade feet and the scores reduced to zero at the end of treatment. There were three recurrences at 6 months follow-up amounting to 1 7% failure rate. Two of them necessitated percutaneous tenotomy of tendoachilles and one underwent posteromedial soft tissue release with good result at end of one year. Ponseti’s method is an effective treatment option in the management of recurrent clubfeet following Kite’s method. Although short term results are promising, larger series with long term follow — up is warranted.
Key words: Clubfoot, Recurrence, Ponseti’s correction, Kite’s cast.
Single stage- single incision correction of congenital vertical talus.
Dr. Ashutosh Bhosale Dr. M. Rajeev Rao,Dr. M. Ramesh, Dr.Manjunath, Dr. Yogishwar
Jubilee Mission Medical College and Research Institute, Thrissur, Kerala, India.
Introduction:
Congenital vertical talus is an exceedingly .rare deformity. Unlike clubfoot, closed treatment with manipulation and casts is rarely successful. Surgery is almost always necessary with consensus regarding open reduction and realignment of talonavicular joint in children below 3 years. There is hardly any consensus regarding incisions used — single or multiple incisions. Even there is no fixed guideline regarding staged procedure or single stage correction.This prospective clinical study evaluates clinical, radiological and functional outcome of single stage- single incision correction of congenital vertical talus.
Results:
Parents were satisfied with appearance of feet with maintenance of longitudinal arch at lX months follow up. Average dorsiflexion was 10 degrees and plantar flexion was 20 degrees. Ten feet were rated good while 3 feet were fair by Adalaar score. Radiologically talocalcaneal and tab-metatarsal alignment was achieved in all cases. There were no complications like skin necrosis and AVN of talus. Push off was oflen a bit weak and plantar flexion was limited in 9 feet.
Conclusion:
Lengthening of toe extensors and peroneals was not required due to early surgeries before walking age. Hence single medial incision was sufficient to achieve reduction. Maintenance of reduction with k wires allows single stage correction. Single incision, Single stage correction of congenital vertical talus has good radiological and functional outcome without any significant complication
Congenital posteromedial bowing of tibia – is early surgery worthwhile?
Dr. Arjun A. Dhawale Dr. Ashok N. Johari, Dr. Abhijit Salaskar, Dr. Alaric Aroojis
E-mail – arjundhawale@hotmail.com
Phone no- 022-24365050
KEY WORDS – congenital posteromedial bowing tibia, surgery
AIMS- To study the natural history and results of conservative and surgical treatment in posteromedial bowing of the tibia.
MATERIALS & METHODS - Twenty cases of posteromedial bowing of the tibia and fibula with mean follow-up of 6.4 years were evaluated with respect to the temporal change in the angles of medial and posterior bowing of the tibia and fibula and limb length discrepancy. 11 cases were managed conservatively and 9 cases were operated. The indications for surgery, modality of treatment and complications are discussed. In the surgical group, osteotomy and K wire fixation was done in 3 cases and osteotomy and Ilizarov lengthening was done in 6 cases. The mean values of medial and posterior angulation and limb length discrepancy at age less than 3 years and age more than 3 years in the conservative and operative groups were compared using statistical analysis.
RESULTS - A statistically significant difference was observed on comparing the mean values of medial and posterior angulation of the tibia and fibula before and after the age of 3 years in the conservative and operative groups indicating a decrease in the bowing in both groups. The LLD increased in the conservative group with age and was corrected in the operative group after surgery. The incidence of complications in the surgical group was high.
CONCLUSIONS- In view of the high incidence of complications due to surgery, we advocate a conservative approach in all patients and a one stage lengthening closer to skeletal maturity.
ROLE OF VASCULARISED FREE FIBULA GRAFT IN CONGENITAL PSEUDOARTHROSIS OF TIBIA-ANALYSIS OF LONG TERM FUNCTIONAL OUTCOME
Dr. Praveen Bhardwaj (Presenting author); Dr. S. Rajasabapathy; Dr. S. Rajsekaran; Dr. Deendayalan; Dr.Hari Venkatramani;
Department of Plastic, Burns, Hand & Microsurgery Surgery
GANGA HOSPITAL
COIMBATORE
INTRODUCTION: Congenital Pseudoarthrosis of Tibia (CPT) has challenged generations of surgeons and the results of various treatment modalities described in past have been disappointing. Microvascular free transfer of vascularized fibula following excision of the pathological segment of the bone has revolutionized the treatment of CPT.
MATERIAL AND METHODS: During the period of 1998 to 2005 we performed Microvascular free transfer of vascularized fibula for 11 cases of CPT. The age at the time of surgery ranged 1 year to 4 years 10 months. In all cases contralateral fibula was used as graft. Follow up averaged 4 years (Range, 1 year to 8 years 2 months).
RESULTS: We obtained satisfactory results in all the cases as assessed by timing of union and deformity prevention/correction. Primary union was achieved in all the cases. Union was evident at average of four months. All the patients were kept on plaster of Paris cast till corticalisation of the transferred fibula was evident, which on an average took about 1 year. The graft was further protected by brace for another two years but full unsupported weight bearing was allowed. Hypertrophy of fibula was evident in all the cases. None of the cases had stress fracture of the fibula. The residual shortening was (<)2 cm and all the patients had almost normal gait. Two patients had valgus deformity of the ankle at donor leg, which required transfixing of the fibula to tibia above the syndesmosis in one case and modified foot wear with medial arch support in another. There was no other significant donor site morbidity in any of the cases.
CONCLUSION: Achieving union is the prime problem in management of congenital pseudoarthrosis of tibia and free vascularized fibula addresses it best. It is a very effective and safe method, and gives superior results as compared to any of the other described modalities, including Ilizarov technique. It is a single stage procedure and patient compliance is good. Union achieved is stronger than after other procedures. Surgery should be done at early age to prevent the secondary deformities like growth abnormalities, abnormal physeal inclination, posterior bowing of the proximal tibia and foot deformities. We believe that if union is achieved early all these secondary problems can be prevented. Although the procedure can be done even in case of multiple failed procedures, it gives best results when done primarily. Man days lost and economical loss because of repeated failed surgeries is enormous. Critical thing is anastomosis, operating in the virgin field gives 100 % good results. We recommend free vascularized fibula as primary treatment for congenital pseudoarthrosis of tibia.
KEY WORDS: Vascularized free fibula; congenital pseudoarthrosis tibia.
EXTENT OF REMODELING OF THE PROXIMAL FEMUR AND ACETABULUM BETWEEN DISEASE HEALING AND SKELETAL MATURITY IN PERTHES’ DISEASE
Hitesh Shah, Siddesh ND, Benjamin Joseph
Kasturba Medical College, Manipal
Introduction:
It is possible that between healing of the Perthes’ disease and skeletal maturity some remodeling of the femur and acetabulum can occur such that further improvement of outcome can occur. Conversely, any aberrant growth that has begun during the active stage of the disease may progress even after healing till skeletal growth is complete. This would cause deterioration of the outcome.
Aims:
This study was undertaken to identify the structural changes that occur in proximal femur and acetabulum between healing and skeletal maturity.
Methods:
40 children with Perthes’ disease were followed up from the point of complete healing of the disease till skeletal maturity.
The following variables were assessed on radiographs at healing and again at skeletal maturity:
The shape of the femoral head
The size of the femoral head
The extent of greater trochanteric overgrowth
Sharp’s angle
The extent of extrusion of the femoral head
Stulberg’s grading of the hip
The following clinical variables were also noted at healing and again at skeletal maturity:
The limb length
Trendelenberg sign
The range of motion of the hip
Results:
The variables fell into three groups; those that improved with growth, those that deteriorated with growth and those that remained unchanged. The factors that were associated with these three groups were identified and the relevance of the effect of remodeling of the hips is discussed.
DONAR SITE MORBIDITY AT TIBIA IN PATIENTS WHO WERE TREATED WITH CORTICAL BONE GRAFT
Siddesh ND, Hitesh Shah, Benjamin Joseph
Kasturba Medical College, Manipal.
Introduction:
Bone grafting is commonly used for the treatment of various conditions in orthopaedics. Cortical and cancellous bone grafts are associated with donor site morbidity. We use the tibial cortical bone grafts for primary treatment of patients with congenital pseudarthosis of tibia.
Aim:
The aim of this study is to evaluate the donor site morbidity and complications when harvesting cortical bone from the medial side of the tibia. In addition to know the compromise of quality-of-life because of tibial cortical bone graft.
Material and methods:
The study is composed of 30 consecutively patients treated with cortical bone graft of tibia. The patients were retrospectively evaluated with regard to postoperative donor site morbidity and complications at the donor site. The medical records of thirty patients who had undergone cortical grafting procedures for the treatment of congenital pseudarthrosis of tibia from 1990 to 2006 were retrospectively reviewed. Demographic characteristics and postoperative complications were recorded. All were evaluated for postoperative and residual pain, functional limitations, cosmetic appearance related to donor site.
Results:
None of the patients has post operative pain more than 3 weeks or has residual pain at donor site. All patients had normal gait after 6 weeks of surgery. One patient had pathological fracture of tibia 3 years after surgery. Pathological fracture was treated with open reduction internal fixation. Sound union occurred after 3 months without complication. 5 patients had anterior bowing of tibia which is not causing functional impairment. No patients have neurovascular complication following cortical bone grafting.
Conclusion:
Harvesting cortical bone graft from tibia is simple method with less morbidity and complication rates. It is associated with minimal compromise of quality of life.
EFFECT OF TROCHANTERIC EPIPHYSIODESIS IN PERTHES’ DISEASE
Hitesh Shah, N.D. Siddesh, Benjamin Joseph
Paediatric Orthopaedics Service
Kasturba Medical College, Manipal.
We evaluated the effect of trochanteric epiphysiodesis in children who had the procedure done during the active stage of Perthes’ disease and have now reached skeletal maturity. All the children included in the study had unilateral Perthes’disease.
Measurements were made on the anteroposterior radiograph of each patient taken at skeletal maturity. The height of the tip of the trochanter in relation to: a) the articular surface of the femoral head and b) the centre of the femoral head were measured. The length of the abductor lever arm was estimated by measuring the horizontal distance between the tip of the trochanter and the centre of the femoral head.
All measurements were expressed as a percentage ratio of the normal value of the unaffected contralateral hip. These measurements were also compared to identical measurements made on untreated patients with Perthes’disease who had reached skeletal maturity.
Our results clearly show that trochanteric epiphysiodesis done in conjunction with a varus de-rotation osteotomy minimizes the risk of trochanteric overgrowth. In the light of our results we recommend that in the older child with Perthes’ disease, trochanteric epiphysiodesis be performed routinely whenever containment surgery is undertaken.
Management of Pink Pulseless Hand in Pediatric Supracondylar Fractures of Humerus.
Dr. Ramesh Perumal
Dr. S Rajasekaran, Dr. Ajoy P Shetty.
Institution:
Department of Orthopedic Surgery,
Ganga Hospital, 313 Mettupalayam Road,
Coimbatore — 641 043. Tamil Nadu, India.
Introduction: The investigations and treatment of supracondylar fractures with :
concomitant vascular compromise is controversial. If the pulse does not return after closed reduction and the hand remains cold and white, exploration of the artery is indicated. The management of children with a satisfactory closed reduction, and an absent radial pulse, but a well-perfused hand, however is debatable. Recommended treatment options include observation, immediate exploration, exploration if the pulse has not returned by 24 hours and immediate angiography. The purpose of our study is to determine the outcome of children with a supracondylar fracture and an absent radial pulse.
Material and Methods: This study group was drawn from:
34 patients seen in our Hospital in from January 2005 to December 2006 with supracondylar fractures. Of this 7 (4.8%) had an absence of a radial pulse with an otherwise well-perfused hand.. All 7 patients in the study group had completely displaced, extension-type injuries. 6boys and a girl ranging in age from 5 years to 1 lyears (average, 8 years) were in this group. two patients had associated neurologic complications, one with median nerve problems and one with anterior interosseous nerve palsy. In all cases, the injury was caused by a fall onto the injured extremity. The initial treatment for those children were immediate closed reduction and 2 lateral k-wire fixation. The pulse and the perfusion of the hand returned to normal in two children but the remaining five children had no palpable radial pulse but a well perfused hand. At final review of 5 patients with pink pulseless hand, no signs suggestive of cold intolerance ,exercise induced ischaemic pain and limb length discrepancy were found. One had cubitus varus deformity and neurological deficits recovered completely.
Conclusion:
In Supracondylar fractures with absent radial pulse, the primary indication for arterial exploration is a cold white hand after closed reduction. An absent pulse however, is not an absolute indication for exploration of the artery, provided the hand remains well perfUsed and a compartment syndrome does not develop
Surgical Stabilization of High Grade Spondylolisthesis in Adolescent Patients; Results and clinico-radiological correlation - A review of 17 cases
Dr Swapnil Keny MS
Dr Ram Chaddha MS
Consultant Pediatric Orthopaedic Surgeon
Consultant Spine Surgeon
Gurunanak Hospital and Research Centre , Mumbai
Introduction:
Surgical Stabilization with interbody fusion is an accepted modality of treatment for grade 2 and grade 3 listhesis in adolescent patients .In this paper we reviewed the surgical resultsl7 patients who had undergone posterior instrumentation and interbody fusion for grade 2 and grade 3 spondylolisthesis and tried to establish a clinical correlation between clinical symptoms and radiological results.
Material and Methods:
We retrospectively analysed 17 adolescent patients who had undergone instrumented posterior lumbar interbody fusion for high grade spondylolisthesis .A detailed history,clinical examination and radiological examination was performed and was compaired to the preoperative case records.
Results:
At a minimum follow up of 5 years. all patients had maintained the achieved correction of the deformity with radiological evidence of fusion. All patients had complete relief of radicular symptoms. However back pain was persistent upto 30 % of patients. Not all children were able to resume their preoperative level of activity due to pain and low back stiffuess.
Conclusion:
Buckling Collapse of the Spine in Childhood Spinal Tuberculosis
Surgical Stabilization of High Grade Spondylolisthesis in Adolescent Patients; Results and clinico-radiological correlation - A review of 17 cases
Presenting Author: Dr. Vijay Kamath
Co-Authors: Dr. S Rajasekaran, Dr. Naresh Babu
Institution: Department of Orthopedic Surgery,
Ganga Hospital, 313 Mettupalayam Road,
Coimbatore — 641 043. Tamil Nadu, India.
Abstract:
We prospectively followed 61 children under 15 years of age at the time of diagnosis to identify the risk factors for deformity progression. The children had 63 lesions and a minimum of 15 years followup. All exhibited an increase in deformity during the active disease phase, but 26 of 63 (41%) continued to progress during the quiescent phase until the growth was complete. In 21 of those 26, there was an increase in angular kyphosis with a final deformity> than 90°. In the other five, the deformity resembled a buckling collapse analogous to failure of an axially loaded slender column; the deformity was more than 100* and associated with facet dislocation at multiple levels. These patients’ vertebral segments above the level of destruction underwent severe sagittal rotation resulting in horizontal vertebrae with vertical growth plates, which resulted in longitudinal overgrowth of the vertebral segments. Risk factors for buckling collapse included an age of less than 7 years at the time of the disease, thoracolumbar involvement, loss of more than two vertebral bodies, and presence of radiographic spine-at-risk signs. Children at risk for buckling collapse must be carefully watched and the spine stabilized to avoid a massive increase in deformity.