Abstracts
-
1. A Short Leg Corrective Brace for Varus Deformity of the Knee in young Children with Rickets
T. Koshino
Summary
Department of Orthopaedic Surgery, Yokohama City University, School of Medicine, Yokohama, Japan.Varus or valgus deformity of the knee was treated with a short leg corrective brace in seven young children (one boy and six girls) with rickets. The brace has an upright medially and a pad for counterpush laterally for correction of varus, and vice versa arrangement for correction for valgus. Sideways pressure was applied by a pad on the lateral side of the lower leg to correct tibia vara. It resulted in satisfactory correction of bow legs in six cases with a mean age at the initial bracing of 2.5 years, while bracing was unsatisfactory for one girl with knock knees.
2. New Measurement of Patellar Height in the Knees of Children Using the Epiphyseal Line MidpointTomihisa Koshino, MD, and Kozo Sugimoto, MD
Summary
Department of Orthopaedic Surgery, Yokohama City University, School of Medicine, Yokohama, Japan.The height of the patella was reevaluated by the ratio of the distance from the center of the patella to the epiphyseal line midpoint in the proximal tibia (PT) to that between the distances of the distal femur and of the proximal tibia (FT) on 59 knees of 36 normal children whose ages ranged from 3 to 18 years (average 10.6 years). The averaged ratio of PT to FT was 1.31 ± 0.9 at full extension and gradually decreased to 0.99 ± 0.06 at 90º flexion. Changes in value were minimal within the range of 0.99-1.20 in the range of knee flexion from 30 to 90º.
Key Words : Child’s knee - Epiphyseal midpoints - Measurements on roentogenogram - patellar height - Ratio of patellotibial distance to femorotibial distance.
3. Avascular Necrosis in ChildrenElhanan Bar-On, MD
AVN in Children May Be:- Transient
- Incomplete
- Segmental
- Lateral Pillar Preservation
Biologic- Perthes
- Sickle Cell; Thalassemia
- Gaucher
- Septic Arthritis / Osteomyelitis
- AIDS
- Steroids (Transplants; SLE; Leukemia)
- Growth Hormone
- Fracture
- Latrogenic
- DDH
- SCFE
- Prevention
Biologic- Steroids
- Growth Hormone
- Perthes
- Sickle Cell; Thalassemia
- Gaucher
- AIDS
- Septic Arthritis
- Gradual Reduction
- Streching of Soft Tissues : Adductors, Iliopsoas, Capsule
- Reduction of Pressure
- Prevention of AVN
- Overhead Adductors
- Introduction in 70’s
- Reduction of AVN (Salter, Gage)
Concomittant Changes in Treatment:
Traction - Efficacy
Gentle VS Forced Reduction - Human VS Frog Position
- Tachdjian 1990 : "The importance of preliminary traction cannot be overemphasized"
- Tachdjian 2002 : "The need for traction in preventing AVN remains unproven"
- General Anesthesia
- Adductor Tenotomy
- Human Position
- Delay to Appearance of Ossific Nucleus
- Adductor + Psoas Release
- Femoral Shortening
- Early Pelvic Osteotomy
- Early Treatment
- Minimal Manipulaion
- Screw In Situ
- Open Reduction
- Late Osteotomy
- Distal to Deformity
- Neck Shortening
- Treatment of Sequelae
4. Ilizarov Hip Reconstruction for the late sequale of septic arthritis and D.D.H.Noam Bor, M.D., Basil Kaufman, M.D.
Introduction
Pediatric Orthopedic Unit and Orthopedic Department, Haememk Central Hospital, Afula -IsraelAcute septic arthritis and developmental dysplasia of the hip (D.D.H.), are very dissimilar. diseases of infancy and childhood. However, they share almost the same long-term severe sequale on the affected hip, resulted in destroyed and deformed femoral head, subluxation or dislocation of the hip, leg length discrepancy.
Many primary and secondary treatments have been proposed including hip arthrodesis, trochanteric advancement, pelvic osteotomy, acetabuloplasty, and femoral osteotomy. Total hip replacement is considered the best solution for the advanced age population, however, has substantial drawbacks on the young age group.
Schanz and others have addressed this problem with a proximal femoral valgus osteotomy, which provides good stability to the unstable hip, but still leaves the affected lower limb short.
The technique developed by Ilizarov, using his apparatus, and according to the biological principles that he elucidated, two main goals of treatment can be addressed : 1. Correction of the instability of the hip. 2. Lengthening and well aligning the affected limb.
We present our experience with this method of treatment during the last 8 years.
Material and MethodsBetween 1996 and 2005 nine patients, 5 males and 4 females, had undergone the Ilizarov hip reconstruction surgery. The overall followup is in an average of 3.9 years (range 1-8). One Patient had the same procedure twice, 3.5 years apart. The etiology for the affected hip was septic arthritis in 5 patients, DDH in 3 patients, and paralytic dislocation of the hip in another patient. According to the classification of Choi (Hunka’s modification), in the patients with the sequale of septic hip, 1 was type II-A; 1 patient type III-A; 2 type IV-A; and I patient type IV-B.
All patients had a very unsightly Trendelenburg gait prior to surgery, and an average of 4.2 cm (range 2-7) of limb length discrepancy. Mean age at surgery was 19.3 years (mean 15-35.5). The Ilizarov apparatus composed of one arch and two rings was applied on all patients. Double level low energy osteotomy was performed :
Proximal subtrochanteric valgus / extension was of an average of 50 degrees (range 20-75), and 20 degrees (range 15-30) respectively. The average stay in the Ilizarov frame was 6.5 months (range 3.5-11).
ResultsThe following complications were noticed : Almost every patient experienced at least one episode of pin tract infection, in one patient a change of an infected pin was required. Three patients were re-admitted to hospital for intravenous antibiotic treatment. Two patients experinced a fracture after frame removal : In one patient, the fracture occurred through the new bone regenerate at the lengthening level, treated with fracture reduction and fixation with Nancy nails. Another patient had a fracture through the proximal valgus osteotomy following a fall in the bathroom, she was treated by open reduction and internal fixation with an AO DCP plate. For poor regenerate at the lengthening site, another patient had undergone at the time of frame removal, a reinforcement of the regenerate with an AO DCP plate, and ticalcium phospate bone substitute. Two patients underwent quadricepsplasty for lack of knee flexion (maximum 30 degrees), 2 and 4 years following the removal of the Ilizarov apparatus. One patient has still knee flexion limitation of up to 60 degrees only. Two patients remained with limb length discrepancy of 2 cm each.
All patients experienced great improvement in their gait pattern, with almost elimination of the characteristic preoperative Trendelenburg gait. The Harris hip score before surgery was 52 (range 30-70), and 72 (range 50-85) after surgery. All patients were pleased with the results of the operation, despite the complications that most of them experienced during and following treatment.
ConclusionAt an average of 3.9 years follow-up, the Ilizarov hip reconstruction surgery for late sequale of
septic hip and DDH has releived symptoms and improved function in the 9 patients operated
upon. However, the morbidity is still significant, treatment time is relatively long, and major
complications are due to happen. It is assumed that few of the above mentioned complications can be avoided like the postopertive restricted knee flexion range of motion, by an intensive physiotherapy during treatment and following the apparatus removal.
The operation is an attractive alternative to hip arthrodesis or total hip replacement which are less applicable to the young population.
This procedure provides stability to the hip, allows restoration of leg length discrepancy, and the correct alignment of the mechanical axis of the limb.
5. Pelvic Osteotomies in the Treatment of Developmental Hip DysplasiaDr. Elhanan Bar-On, MD
D.D.H. - Treatment Principles 3 Stages :
- Reduction
- Stabilization
- Biomechanical Improvement
- Decreased Weight Bearing Area
- Increased Pressure
- Early Osteoarthritis
Biomechanical Improvement
- Prevention
- Delay of Osteoarthritis
- Alleviation of Present Symptoms
- Increased Bone Stock for THR
Symptoms
- Pain
- Fatigue
- Snapping
- Limp
- Trendelenburg
- Shortening
- Limited ROM
- Acetabulum
- Femur
- Acetabulo-Femoral Relationship
- Associated Deformities
Acetabulum
- Depth Idelberger & Frank Angle (<)50º
- Orientation Sharp's Angle (<)40º
- Sourcil Angle (<)10º Anteversion / Retroversion
- Size
- Sphericity Mose
- Neck Size & Orientation
- Coxa Valga / Anteversion
- Trochanteric Height - ATD
- Acetabulo - Femoral Relationship
- Static Coverage
- Lateral : Center - Edge
- Angle >20º Coverage > 85 %
- Trochanteric Height - ATD
- Anterior : Faux Profil Angle >20º
- Dyanamic : Congruency
- Labral Tears
- Soft Tissue Contractures
- Leg Length Discrepancy
- Spinal Deformity
- Previous Surgery
- Pelvic Obliquity
Problems Addressed
- Coverage
- Congruency
- Intra-articular Pathology
- Range of Motion
- Abductor Weakness
- Leg Length Discrepancy
- Pelvis
- Femur
- Soft Tissues
- Volume Augmentation
- Volume Reduction
- Redirectional
- Colonna (1951); Colonna Arthroplasty
- Shelf Arthroplasty Shelf Procedure
- Weakness till Consolidation
- Graft Resorbtion
- Non Cartilaginous Coverage
- Chiari : Chiari Osteotomy
- Verticalization of True Joint
- Growth Arrest at Acetabular Rim
- Non Cartilaginous Coverage
- Pemberton
- Dega
- Single (Salter)
- Double (Sutherland)
- Triple (Steel; Tonnis)
- Periacetabular (Wagner; Ganz)
- Correction Ability VS
- Technical Difficulty
Disadvantages
- Correction up to 15º
- Limited Correction in Older Patients
- No Joint Medialization
Disadvantages
- 3 Incisions - Excessive Dissection
- Pelvic Ring Disruption
- Ischial Cut Inaccessible During Manipulation
Disadvantages
- Contraindicated in Open Triradiate Cartilage
- Deep, Blind Cuts
- Narrow Safety Margin
- Difficult C-arm Imaging
- High Radiation
- Wide Dissection
- Technically Demanding
Redirectional Osteotomies
Complications
- Nerve Injury (LFC, Femoral, Sciatic)
- Joint Penetration
- Narrow Safety Margin
- AVN of Acetabulum
- Non Union
- Abductor Weakness
- New Surgical Approaches
- Arthroscopic Assisted Osteotomies
- Electrophysiologic Monitoring
- Navigation Systems
- Chiari - Incongruous Joint Neuromuscular Patient
- Salter - Small Correction, Young patient
- Triple - Congruous Joint, Open Triradiate Cartilage
- Periacetabular - Congruous Joint, Closed Triradiate Cartilage
- Varus + Derotation—> Increased Coverage
- Valgus + Flexion // Extension for AVN
- Trochanteric Transfer
- Length Equalization
Reduction of Soft Tissue Dissection by:
- New Surgical Approaches
- Navigation Systems
- Arthroscopic Assisted Osteotomies
Limitations
- One Plane at a time
- No Transverse Plane
- Radiation Dose (Patient & Surgeon)
- Cumbersome Equipment & Draping
- Heavy Lead Gown
- Simultaneous Multiple Plane Viewing
- Decreased Radiation
- Additional Intraoperative Data
- 3D orientation
- Decreased Soft Tissue Dissection
- Decreased Radiation
- Increased Safety Margin
- Additional Intraoperative Input (CT; MRI)
- Increased Accuracy of Osteotomies
- Increased Accuracy of Correction & Fixation
- Patient Selection
- Fiducial Screw Placement
- CT Scan + Transfer to Navigator
- Image Registration
- Osteotome Calibration
- Navigate & Osteotomize
- Long Learning Curve
- Radiation (CT)
- Cumbersome Registration & Screw Placement
- Multimodality Navigation
- Continued Navigation after Fragment Mobilization ?Unresolved ?
- Treatment of Late Diagnosed DDH
- Treatment of Asymptomatic Dysplasia
- Actual Long Term Benefit
- Obstetric Problems
- Continue Follow Up Until Skeletal Maturity
6. Result of limb salvage treatment for congenital tibial hemimelia
Toshio Fujii
Department of Orthopaedic Surgery, Fukruoka Children’s Hospital, Fukuoka, JapanThe purpose of this paper is to clarify the results of limb salvage treatment for congenital tibial hemimelia.
The treatment of congenital tibial hemimelia is controversial, and many reports have been in favour of early knee disarticulation for the total absence type, and tibiofibular fusion and syme’s amputation for partial absence type.
For the limb salvage treatment, we performed reconstruction of knee and ankle, and repeated lengthening of femur or fused fibula throughout childhood. For partial absence of the tibia, we performed tibiofibular fusion and ankle plasty. After posteromedial release of the foot, we put the distal end of fibula into calcaneus preserving distal epiphysis of fibula to get good longitudinal growth of the fibula after surgery. For total absence of the tibia, we performed modified Brown’s centralization of fibula and ankle plasty. Leg lengthening was repeated through childhood on either femur or fibula.
The materials were nine limbs out of seven children. They were four legs with distal partial absence of tibia and five legs with total absence of tibia. Two children had right partial absence and left total absence. Age at the first surgery ranged from 5 months to 5 years and 11 months and the average was 2 years.
The age at the follow-up ranged from 7 years to 21 years and the average was 7 years. At the follow-up, all the patients are ambulating with AFO and going to school without crutches. In conclusion, limb salvage treatment for congenital tibial hemimelia is an acceptable procedure and has great possibility to achieve good ADL.
7. Surgical Treatment of Congenital Dislocation of the Patella
Toshio Fujii, Haruhisa Yanagida, Akifusa wada, Kazuyuki Takamura
Department of Orthopaedic Surgery, Fukuoka Children’s Hospital, JapanCongenital dislocation of the patella requires early surgical reduction for better walking. The purpose of this paper is to clarify the results of our combined soft tissue procedures.
We reviewed 6 knees in 5 children. The age at surgery ranged from 3 to 12 years. The mean follow-up period is 7 years. The surgical procedures involve lateral release, resection and tightening of medial capsule, semitendinosus muscle transfer to the patella. Quadriceps lengthening was also required in two knees.
Five knees operated on less than 5 years of age were well reduced and well positioned in the femoral groove at follow-up. One knee operated at the age of 12 years showed subluxation. Episodes of giving way and abnormal gait disappeared after surgery in all patients.
We found that the transferred semitendinosus muscle acts as a dynamic tenodesis to maintain good patellar position during knee flexion. Femoral groove depth increased after surgery. The improvement in the young infants was better than in older child. In conclusion, early surgical reduction is extremely important and it will stimulate proper development of femoral groove. Semitendinosus tendon transfer combined with lateral release is effective to keep the patella in its groove during knee flexion even in the child with abnormal joint laxity.
8. Results of hip abduction brace (Nishio ! Cs Brace) for LCPD
Yutaka Oketani, Toshio Fujii, Akifusa Wada
Purpose:
Department of Orthopaedic Surgery, Fukuoka Children’s Hospital, JapanTo report the results of the non-weight bearing hip abduction brace (Nishio ! Cs Brace) for unilateral Legg Calve Perthes disease.
Materials:We studied 98 hips that were treated by Nishio ! Cs brace that contains the femoral head in the acetabulum at 30 degrees hip abduction and has a pole beneath the sciatic tubercle for the non-weight bearing of the hip. Average age at the time of first visit is 6.5 years, and at the last visit was 13.0 years. We evaluated hips with Catterall classification, lateral pillar classification and Stulberg classification.
Results:The Catterall classification judged when the period ended dividing (passage of nine months on the average from the first medical examination) showed in two hips type 1, 37 in type 2, 40 in type 3, and 19 in type 4. The lateral pillar classifications showed eight hips in group A, 55 in group B, 22 in group B/C, and 13 in group C. the Stulberg classification when the final passage was observed 26 hips in the type 1, 40 in type 2 and 21 in type3 9 in type 4 and 2 in type 5. Namely, 67.3% (66/98 hips) showed satisfactory results.
Conclusion :Nishoi Cs brace is satisfactorily effective for the treatment of LCPD.
9. Surgical Treatment of Congenital Dislocation of the Patella
Toshio Fujii, Haruhisa Yanagida, Akifusa wada, Kazuyuki Takamura
Department of Orthopaedic Surgery, Fukuoka Children’s Hospital, JapanCongenital dislocation of the patella requires early surgical reduction for better walking. The purpose of this paper is to clarify the results of our combined soft tissue procedures. We reviewed 6 knees in 5 children. The age at surgery ranged from 3 to 12 years. The mean follow-up period is 7 years. The surgical procedures involve lateral release, resection and tightening of medial capsule, semitendinosus muscle transfer to the patella. Quadriceps lengthening was also required in two knees.
Five knees operated on less than 5 years of age were well reduced and well positioned in the femoral groove at follow-up. One knee operated at the age of 12 years showed subluxation. Episodes of giving way and abnormal gait disappeared after surgery in all patients.We found that the transferred semitendinosus muscle acts as a dynamic tenodesis to maintain good patellar position during knee flexion. Femoral groove depth increased after surgery. The improvement in the young infants was better than in older child. In conclusion, early surgical reduction is extremely important and it will stimulate proper development of femoral groove. Semitendinosus tendon transfer combined with lateral release is effective to keep the patella in its groove during knee flexion even in the child with abnormal joint laxity.
10. Results of hip abduction brace (Nishio ! Cs Brace) for LCPD
Yutaka Oketani, Toshio Fujii, Akifusa Wada
Purpose :
Department of Orthopaedic Surgery, Fukuoka Children’s Hospital, JapanTo report the results of the non-weight bearing hip abduction brace (Nishio ! Cs Brace) for unilateral Legg Calve Perthes disease.
Materials :We studied 98 hips that were treated by Nishio ! Cs brace that contains the femoral head in the acetabulum at 30 degrees hip abduction and has a pole beneath the sciatic tubercle for the non-weight bearing of the hip. Average age at the time of first visit is 6.5 years, and at the last visit was 13.0 years. We evaluated hips with Catterall classification, lateral pillar classification and Stulberg classification.
Results :The Catterall classification judged when the period ended dividing (passage of nine months on the average from the first medical examination) showed in two hips type 1, 37 in type 2, 40 in type 3, and 19 in type 4. The lateral pillar classifications showed eight hips in group A, 55 in group B, 22 in group B/C, and 13 in group C. the Stulberg classification when the final passage was observed 26 hips in the type 1, 40 in type 2 and 21 in type3 9 in type 4 and 2 in type 5. Namely, 67.3% (66/98 hips) showed satisfactory results.
Conclusion :Nishoi Cs brace is satisfactorily effective for the treatment of LCPD.
11. Co-relation between Congenital Vertebral Anomalies and other Congenital Anomalies
Yutaka Oketani, Haruhisa Yanagida, Ken Wada, Toshio Fujii
Purpose:
Department of Orthopedic Surgery, Fukuoka Children’s Hospital, JapanTo clarify the co-relation between congenital vertebral anomalies and other congenital anomalies.
Materials and Methods:We reviewed 1,520 children who had congenital vertebral anomalies from 1980 - 1997, and surveyed Co-relation Between Congenital Vertebral Anomalies and Other Congenital Anomalies. Among of them, 133 children had congenital vertebral anomalies, 965 cases had cardiac anomalies, 248 had pediatrics or pediatric surgery.
12. Fracture Neck of Femur in Children
Dr. K. P. Srivastava, Prof. Emeritus of Orthopaedics
Fracture likely to be missed due to:
Fractures of the proximal femur are uncommon in children.- Undisplaced Fracture
- Associated fracture of pelvis
- Associated epsilateral limb fracture
- Associated Head Injury
Due to direct blow on the greater trochanter or in a car accident where the child is sitting in the car in full extension to the knee joint. Another cause in our country is fall from height (trees, bicycle, etc.). A number of femoral neck fractures in children are associated with multiple injuries. The mechanism is different in elderly people where external rotation, abduction and extension forces cause the femoral neck fracture.
Difference with adults:- Trabecular pattern is not along the stress lines.
- Fracture is usually transverse with smooth fracture surface therefore closed reduction is less stable.
- Growth disturbance may occur due to the involvement of femoral and trochantric epiphyses.
- Coxa vara and avascular necrosis are more common in children and difficult to manage.
- Displaced without dislocation of head of femur - Closed reduction and multiple screw flxation
- Displaced with dislocation of head of femur - Open reduction and multiple screw fixation Primary Osteotomy, as AVN is inevitable
- Commonest 50%
- 40% Incidence of Avascular Necrosis
- Degree of displacement determines the prognosis
- Reduction & Cannulated screw fixation
- Gentle closed attempt, if fails, open by Watson Jones approach
- Aspiration is essential - 4.5 cannulated screws with washer are used for the internal fixation.
- Second most common fracture
- Prognosis is better than Transcervical fracture.
- Substantial risk of avascular necrosis unlike fractures in adults.
- Undisplaced - Traction or spica in abduction
- Displaced - Internal fixation to avoid redisplacement and coxavara
- Rare Fractures - 2-7 %
- Less Problematic
- Non Union does not occur
- Avascular Necrosis can occur
- alunion is the main problem
- Essentially Conservative (Traction followed by spica)
- If fails, open reduction and fixation by Cannulated screws, compression screw and plate.
- Non Union
- Premature Epiphyseal closure
- Avascular Necrosis
- Varus or Valgus deformity
- Limb Length Discrepancy
- Degenerative Arthritis
- LAM (1971) 13.0 %
- GUPTA & PRUTHI (1976) 17.5 %
- RATLIFF (1981) 10.0 %
- CAMPBELL CLINIC SERIES 06.5 %
- Complete Epiphyseal
- Closure :- Overgrowth of the greater trochanter
- Partial Closure :- Varus or Valgus Deformity
Most Common complication; more than 80% in Epiphyseal Fractures: 50% in Trans-cervical; 25-40 % in Cervico Trochantric or Basal Fractures
- Directly related to initial displacement and compromise of the blood supply at the time of fracture (69%)
- Even undisplaced Type I, II & III fractures can develop avascular necrosis (31%)./
- AVN develops more quickly than adults.
32 children with fracture neck of femur transcervical (18) and basal fractures (14) were included in our series. Age ranged from 1-15 years, with male preponderance. Eight patients had associated multiple injuries.
Type of Fracture:Type No. of patients Percent (%) Epiphyseal Nil Nil Transcervical 18 57.6 Basal 14 42.4 All the patients were treated by gentle reduction and stable internal fixation by AO cannulated lag screws with washer. Caution was taken so that the tip of the screw did not cross the epiphyseal plate. Aspiration of the Haematoma was done prior to surgery to decrease the temponade.
We had total of 6 cases of avascular necrosis (18.69%) and 3 cases of non union (9.37%). It is recommended that all fractures of the femoral neck in children, whether displaced or undisplaced should be treated by internal fixation by lag screws to minimize complications. The washers must be used to achieve compression effect at the site of fracture.
Procedure:Closed reduction was achieved in almost all cases by gentle traction, abduction and internal rotation and the position checked under image intensifier.
The fracture haematoma was aspirated in all the fresh cases at the time of admission.
A lateral incision starting from the greater trochanter 4-5 cms downwards was given and fascia lata and vastus lateralis split. A guide wire was passed on the anterior surface of the neck of femur to get an idea of the angle of anteversion. Drill hole is made on the lateral cortex of the proximal femur under image intensifier, a guide wire is passed over which AO cannulated drill bit was used taking all precautions not to cross the epiphyseal plate. The drill hole is tapped and appropriate size of screw with washer is inserted.
The number of screws (1.2 or 3) and the diameter (4.0 mm or 6.5 mm) depends upon the capacity of femoral neck.
Post Op Management:- Non weight bearing exercises are started from 2nd post operative day and continued for atleast 3 months. Weight bearing is allowed after radiological assessment usually after 3 months.
- Screws are usually removed by the end of 1 year after operation.
- Perfect Reduction is mandatory
- Stop short of epiphyseal plate
- Weight bearing allowed only after radiological union
- Two screws are adequate.
- Removal of screws not before one year.
The average period of follow-up ranged from 3 months to 5 years. Average 2.4 years.
Complications:
Results:Complications n = 18 Transcervical n = 14 Basal n = 32 Total No. of Patients % No. of Patients % No. of Patients % AVN 06 33.33 Nil - 06 18.69 Non - union 03 16.66 Nil - 03 9.37 Coxa-Vara 02 11.10 02 14.28 04 12.50 Coxa-Valga Nil - Nil Nil - Limb-Length Discrepancy 01 05.55 02 04.28 03 9.37 The Overall incidence of Avascular Necrosis was 18.69% and Non Union 9.37% all found in transcervical fractures.
Old Fractures:- Old fractures with non union and avascular necrosis can be treated by sub-trochantric osteotomy (Ratiff).
- Some do primary intertrochanteric osteotomy in anticipation of future complications remodeling of proximal femur in children has been reported (Gupta & Pruthi).
- Gupta & Pruthi (1974) studied results of primary osteotomy in 86 cases (57 Transcervical & 29 cervicotrochanteric or basal fractures).
- Remarkable remodelling of upper end of femur takes place with growth and fracture unites in many cases after intertrochanteric osteotomy (Gupta & Pruthi - 1974).
- Some shortening is not incompatible with good functional results :- Gratifying results (Ratliff 1962).
- Perfect reduction and stable fixation till the fracture unites can prevent non-union in children’s hip fractures.
- The incidence of avascular necrosis can be minimised by proper care in open reduction by avoiding postero superior aspect of neck of femur.
- Also early decompression of tamponade by limited anterior capsulotomy or aspiration is helpful.
Early aspiration with early internal fixation by cannulated screws with washer gives good results in transcervical and basal type of femoral neck fractures.The internal fixation should be done in undisplaced fractures also to prevent displacement. The screws should not cross the epiphyseal plate. Basal fractures have a better prognosis than the transcervical fractures but complications like AVN and Non-union are higher as compared to basal fractures in adults. The treatment of choice in these fractures is also internal fixation. The decreasing incidence is due to perfect reduction & proper internal fixation by cannulated hip screw or compression hip screw with side plate.
Plan of treatment of femoral neck: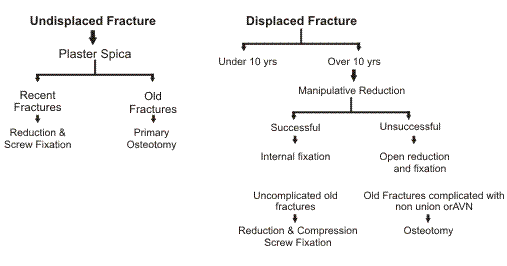
13. Botulinum Toxin in Cerebral Palsy
Dr. K., Vinodh, G.K.N.M Hospital, Coimbatore
Cerebral palsy develops as a result of non progressive injury to the developing CNS. Optimal management of this condition is expensive and requires a muiltidisciplinary approach. Chemo denervation is an important modality in the treatment of spasticity. Alcohol, phenol and botulinum toxin are the three commonly used agents of chemo denervation.
Sero type A of the botulinum toxins is the most potent biologic toxin known to man. First clinical trial of BTX A in C.P. was conducted in 1988. Since then several studies have confirmed the efficacy and safety of this toxin in C.P. BTX A acts in the neuromuscular junction and blocks the neuromuscular transmission, thereby causing temporary partial paralysis of the injected muscle. It is superior to phenol and alcohol in that it diffuses well and does not cause muscle fibrosis.
Indications in C.P.- Dynamic deformity
- Pain
- Symptomatic dystonia
- Diagnostic trial for surgery
- Drooling reduction
The ideal target is a muscle with dynamic posturing with good passive ROM.
Contra indications:- Child less than 18 months old
- Known allergic reaction to BTX
- Significant muscle weakness
- Fixed contracture
The toxin should be stored in freezer and reconstituted with saline just before injecting. The dose is 2-4 units/kg/muscles and the maximum dose is 12-15 units/kg. wt. The toxin is to be injected as close to the neuromuscular junction as possible. For most muscles localization is done by direct palpation. For deeper muscles localization can be done using u/s scan or EMG. In young children the injection is carried out under sedation or a short general anaesthetic.
Duration of action:It usually takes 5-6 months for the action to wear off. In about 10% of patients long term effect is seen.
Complications:There are very few complications. Mild soreness around the injected site for one or two days is noticed. Anti bodies are formed with higher doses and frequent injections. Botulinum toxin can be a useful agent for reducing muscle tone in carefully selected patients.
14. Selective soft tissue release preserves growth plate architecture during limb lengthening
Sabharwal, S., R. D. Harten, et al. (2005)
(Journal of Pediatric Orthopedics 25(5): 617-22)Although distraction osteogenesis has proven successful in children, concerns remain regarding potential growth inhibition of the lengthened limb. Twenty-one 8-week-old New Zealand White rabbits underwent a unilateral 40% tibial lengthening with the contralateral tibia as control. The animals were divided into Achilles tendon release and non-release groups Radiographs and histomorphometric analysis of the proximal tibial growth plate was performed 5 and 10 weeks after distraction. The corrected length of tibias without tenotomy was significantly shorter than the contralateral controls, whereas those with tenotomy were statistically equivalent to the contralateral control tibias. Histologically, the operated limbs without tenotomy showed a significant decrease in thickness and loss of cellular architecture of the proximal tibial growth plate compared with the tenotomy groups, which were of near-normal appearance. A concomitant tendo Achilles lengthening performed with 40% tibial lengthening preserves proximal tibial growth plate architecture in this model.
15. Growth patterns after lengthening of congenitally short lower limbs in young children
Sabharwal, S., D. Paley, et al. (2000)
(Journal of Pediatric Orthopedic 20(2) : 137-45)The purpose of this study was to assess growth patterns after lengthening of the congenitally short femur or tibia in children younger than 6 years. Twenty such children underwent 28 bone segment lengthenings (13 femora and 15 tibiae) by distraction osteogenesis. Our results show that femoral lengthening in children younger than 6 years does not lead to growth ihibition, whereas isolated femoral lengthening may be associated with growth stimulation. Isolated tibial lengthening in children younger than 6 years does not lead to growth inhibition, whereas simultaneous femoral and tibial lengthening or two tibial lengthenings in close succession can lead to tibial growth inhibition.
16. Congenital Radio - Ulnar synostosis Rotation Osteotomy with the llizarov Ex. Fix Report of 4 cases
Micha Rinot, M.D.; Noam Bor, M.D.; Kaufman Basil, M.D.
Orthopedic Department, Hand and Pediatric Orthopedic Units. Central Emek Hospital, Afula - IsraelCongenital radioulnar synostosis is a relatively rare anomaly of the upper extremity with approximately 350 cases reported in the literature. The disability is most significant in bilateral cases with severe pronation. The patient is unable to compensate with scapular and glenohumeral motion. Significant functional difficulty, especially with activities requiring supination is noticed. Attempts to obtain and maintain motion by excision of the synostosis are usually unsuccessful, the synostosis tends to reform despite excision. Gradual correction using the llizarov external fixation, following an osteotomy at the synostosis site, decreases the risk of neurovascular-compromise, and allows the patient to select the functional position.
Material and MethodsIn our study 3 boys and one girl, with a mean age of 11 years (9 to 12.5), underwent surgery since 2001. 3 patients had bilateral deformity, one patient had his only Rt. forearm involved. All patients were followed up for a mean of 44 months (33 to 54). The mean preoperative pronation deformity was 70 degrees (30 to 110). All the three bilateral cases, had their surgery on the non-dominant forearm, the patient with the monolateral deformity preferred to have the surgery on his right dominant hand. All forearms were classified as type 111 according to Cleary and Omer, with visible osseous synostosis associated with posterior dislocation of a hypoplastic radial head.
Operative techniquesThe osteotomies were performed at the level of the synostosis. A three ring llizarov external fixator was applied on the forearm. The correction of the deformity was performed gadually, at a rate of 1 mm a day, by turning proper nuts incorporated in a special rotational construct.
ResultsBone union was achieved in all patients. The mean supination position of the forearms achieved at the end of the correction was 15 degree (0-30). All llizarov frames were removed after an average of 66 days ( 65-71). Immediate postoperative neuropraxia of the radial nerve was noticed in two patients, all recovered completely down the road. One patient developed pin tract infection, treated successfully with oral antibiotics. All patients were extremely satisfied with the result of the surgery. Functional improvements in ADLs were achieved in all patient.
ConclusionThe use of an llizarov external fixation for gradual correction of hyperpronated forearms in radioulnar synostosis, is a safe procedure avoiding tension on vascular and fibrous structures. Surgical approch is minimal, the use of internal devices is avoided.
17. Multiplanar Deformity Analysis of Untreated Blount’s disease
Sanjeev Sabharwal, MD; James Lee Jr., MD, C Zhao, MD.
Introduction:Although varus malalignment of the proximal tibia is the primary pathology in Blounts disease, other limb deformities do exist. Our goal was to determine the occurrence of multiplanar deformities in patients with Blounts disease and whether differences exist between Early Onset and Late Onset forms of the disease.
Materials & Methods:40 patients (60 limbs) including 16 children (26 limbs) with Early Onset and 24 (34 limbs) with Late Onset Blounts disease who had not any prior treatment were identified. Average age at examination was 4.5 years for Early Onset and 12.7 years for Late Onset group. Multiplanar deformity analysis was performed using clinical exam. (Thigh-foot angle (TFA) and passive internal and external hip rotation (IR/ER)) and radiographs (Standing long cassette AP view, AP and lateral views of tibia and scanogram). Frontal plane deformity analysis included radiographic measurement of mechanical axis deviation (MAD), neck-shaft angle, lateral distal femoral angle (LDFA), medial proximal tibial angle (MPTA), lateral distal tibial angle (LDTA) and limb length discrepancy. Sagittal plane analysis included measurement of posterior distal femoral angle (PDFA), posterior proximal tibial angle (PPTA) and anterior distal tibial angle (ADTA). Data analysis was performed using ANOVA and correlation statistics.
Results:
Frontal Plane:Compared to controls, affected Early Onset extremities had 59 mm greater MAD, similar Neck-shaft angle, similar LDFA (m), 12o greater Joint.
Convergence angle, 23o lower MPTA, similar LDTA, 18o greater meta-diaphyseal angle, 3 mm higher fibular elevation. The Late Onset group had 71 mm greater MAD, similar Neck-shaft angle, 6o greater LDFA (m), similar Joint Convergence angle, 12o lower MPTA, similar LDTA and unchanged fibular elevation. Based on scanogram the average shortening of the affected limb was 23 mm in Early Onset and 21 mm in Late Onset patients.
Sagittal Plane:Compared to controls, affected Early Onset extremities had similar PDFA, 18o lower PPTA and similar ADTA. The Late Onset group had similar PDFA, 8o lower PPTA and similar ADTA.
Axial Plane:Compared to controls, affected Early Onset extremities had similar passive Internal/External hip rotation and 27o greater Internal Tibial Torsion. The Late Onset group had similar passive Internal/External hip rotation and 14o greater Internal Tibial Torsion. There was a strong correlation between increasing MAD and worsening MPTA, PPTA and TFA in both groups.
Conclusion:Although both groups with Blounts disease exhibited multiplanar tibial deformities including proximal varus, procurvatum and internal torsion, Early Onset patients had greater severity compared to Late Onsets. Unlike Early Onset group, in Late Onsets one-third of the varus malalignment of the limb was attributed to the distal femur. Neither group showed any significant hip deformity nor sagittal plane malalignment of the distal femur or distal tibia.
Significance:For comprehensive evaluation, multiplanar deformity analysis should be routinely performed when examining a child with Blounts disease.
18. Primary open reduction through an anterior approach for neglected congenital dislocation of the hip
Dr. Koji Noyori
Background:The early detection and treatment before the age of walking is the best approach to the congenital dislocation of the hips. Unfortunately, the dislocation is sometimes discovered by limping after the child starts to walk. Conventional conservative treatment such as Pavlik harness and/or overhead traction is difficult for these cases. Even more, most of them has high dislocated hip, which is too hard to be reduced through a medial approach according to contracture of capsule and abductors. We started to operate high dislocated hips through anterior approach to release of the contracture. Aim of this work was to evaluate the results of primary open reduction with circumferential capsulotomy through an anterior approach performed on seventeen neglected congenital dislocations of the hip after the age of walking.
Material and Methods:We studied 60 hips of 59 patients who visited our clinic between 1987 and 2002 and were diagnosed as congenital dislocation of the hips without previous treatment. The series includes 17 hips of 16 patients who complained of limping after they started walking except two cases who had neurological deficit and malformations. The average age at first-visit was one year eleven months. The average length of follow-up was seven years. The roentgenograms were assessed.
Result:According to Severin's classification. 36 hips were rated as class I, 13 as class II, 9 as class III, and 2 as class IV, which were reduced surgically. Before anterior open reduction, the average acetabular angle was 36 degrees and the average center-edge (CE) angle was -41 degrees. At latest follow-up, the average acetabular angle was 19 degrees and the average CE angle was 21 degrees. The average teardrop distance (TDD) was 23 mm before open reduction and 11 mm at follow-up. At first visit, the affected epiphysis was smaller than the opposite epiphysis. Whereas there were not severe short or valgus neck. At latest follow-up, eighteen femoro-valgus hips and smaller epiphysis were in eleven hips. But flattened or oval head was not shown.
Conclusion:Concentric reduction was obtained even in the high hip dislocations. Growth disturbances of the femoral head did not associated with even if the femoral head was high before anterior open reduction. In two cases acetabular dysplasia did not recover as yet, and needs careful follow-up.
19. Indications for, and Limitations of Kameshita's Conservative and Surgical Treatment of Congenital Clubfoot
Background:We have done Kameshita's conservative and surgical treatment of congenital clubfoot from 1989. The purpose of this paper is to indentify the indications for, and limitations of Kameshita's Treatment.
Material and Methods:Of the 274 patients with 406 clubfeet attending from 1989 to 1999, 142 patients with 204 idiopathic clubfoot treated by same method but not in our clinic.
Results:The foot deformity was classified as mild (28 feet; 14% of 204 feet), moderate (113 feet; 55%), or severe (63 feet; 31%) We classified results after the atraumatic cast treatment as follows. In group A 116 feet; 57% of 204 feet, correction was excellent. In group B 32 feet; 16%, correction was acceptable. In group C 56 feet; 27%, correction was unsatisfactory. For all patients in group A and B 148 feet; 73% of 204 feet, orthotic advised was after cast treatment. For all patients in group C, after atraumatic cast treatment early posteromedial release was done after the age of 6 months. We did calcaneocuboid joint release as well. Fifty-two feet (26%) in group A and B were remedied by conservative treatment. The other 96 feet (47%) in groups A and B had recurrences, and 83 of these feet (41%) were treated by late posteromedial release. Of 139 feet treated surgically, 10 feet (14%) had recurrences. None of the 67 feet treated by posteromedial release with calcaneocuboid joint release had recurrences at the mean follow-up time of five years.
Conclusion:Without talocalcaneal joint release, satisfactory correction could be obtained by posteromedial release with calcaneocuboid joint release, which maintains correction well.
20. Femoral neck anteversion in DDH
Vrisha Madhuri, Harry Fernandez, Gopikrishna, Shyamkumar NK
Introduction and aim:
Department of Orthopaedics and Radiology, Christian Medical College, VelloreFemoral neck anteversion in DDH is considered as one of the factors important to surgical technique and redislocation. In older children a derotation osteotomy is carried out to correct this anteversion during the surgical procedure. The assessment of this anteversion is done clinically by measuring the amount of internal rotation required to achieve a stable contained hip. Recent literature suggests that femoral anteversion is normal in young children with DDH. Conflicting literature exists regarding presence of acetabular anteversion in young children with DDH. This study was carried out to assess femoral anteversion in DDH.
Patients and method:20 children (mean age - 3 years) with 15 normal and 25 affected hips with DDH were evaluated. The affected hips were either dislocated (17) or reduced surgically with in one year ( 8 hips).
The children were divided into 3 age groups less than 2 year, 2 -5 year and more than 5 year. The anteversion of femoral neck on both affected and normal side was measured by computerized tomography using Murphy’s method.
The results showed a mean femoral neck anteversion (affected and unaffected) of 28.25 degrees (SD 10.2). The mean anteversion was 33.6 on dislocated and 27 degree on uninvolved side.
In children less than 5 years there was no significant difference between the involved or uninvolved side. In children over 5 years there was a significant increase (mean - 13.25 degree) in the anteversion angle.
In the post reduction group there was a significant decrease in the anteversion angle suggesting that anteversion decreases after reduction even within 1 year.
The findings suggest that femoral anteversion is normal at birth, the decrease which normally occurs does not occur in hips which continue to remain dislocated. Reduction of the hip causes the anteversion to decrease significantly within 1 year of reduction in young children. In children over 5 years significant degree of anteversion persists and needs to be taken into consideration when planning treatment.
21. Management of Paralytic Foot
Dr. R. A. Agrawal, M.S. (Ortho)
Introduction:
Agrawal Orthopaedic Hospital, GorakhpurDeformities in polio are mainly caused by imbalance in muscles either due to partial or complete paralysis of muscles. Deformities are also caused due to shortening of limbs. In correction of deformity of foot one should have thorough knowledge of the biomechanics of the foot. Biomechanics is the branch of mechanics (i.e. Physics) which interprets static, kinematics, and kinetic human phenomena. In other words biomechanics studies the conditions, when a human body is in state of balance (static), when it moves (kinematics), when it produces some force action and undergoes through the action of force (kinetic). lt is mandatory that the body should be examined as a whole because some deformities are favourable for the patient, e.g., the equinus deformity of the foot associated with shortening of leg is good for patient until the factors causing the deformities are eliminated by lengthening. The deformities of the foot are broadly divided into three planes (a) frontal plane (b) sagittal plane(c) horizontal plane.
Sagittal plane deformities:- Equinus
- Equino-cavus
- Pes planus
- Calcaneus
Viewed from back
- Heel varus
- Heel valgus
Viewed from front
- Supinated foot
- Pronated foot
Viewed from top
- Adducted foot
- Abducted foot Generally deformities are found in combinations such as equino-cavo-varus, plano-valgus etc.
The deformities are corrected by gradual and controlled stretching of soft tissues, tendo Achilles per cutaneus tenotomy either by single stab or double stab, sometimes VY plasty is performed. First the deformities of the fore foot (pronation / supination) is corrected followed by correction of adduction or abduction deformity, next correction of hind foot deformity at the last equinus deformity is corrected. If associated with shortening of leg, simultaneously lengthening of bone is done.
Method:Method by llizarove technique: Usually two rings are placed in tibia and if there is associated limb shortening three rings are placed. One half ring is placed in calcaneus, one half ring Is in the fore foot. In the cases of rotational deformities one half-ring / full ring may be placed in the mid foot and one full ring at the fore foot. All rings are connected to bone with wires and with each other with rods and hinges. Deformities are gradually corrected by distraction at the rate of 1 mm per day.
Result:Results are good as there are less chances of recurrence of deformities, there is no chances of fibrosis because no internal surgery is performed, Joint motions are not affected as no bony surgery is performed, Complications like pin tract infection and pain are common which clear after removal of pins after the removal of frame.
22. Spastic Foot
Dr. K. Vinodh, G.K.N.M Hospital, Coimbatore
In cerebral palsy, the feet may develop any of the various deformities described below. In most of these children, when they begin to walk feet are in mild equinus and varus or valgus. between 2 to 5 yrs the deformity may get better or worse. After 5 to 7 yrs the deformity gets stabilised and deteriorates during adolescence. In diplegics the deformity is usually valgus and in hemiplegics it is equinovarus.
Equinus:Features : Toe walking, early heel raise, contributes to the development of valgus deformity.
Treatment:Serial casting, Botox - 5-6 yrs; Gastroc lengthening - >6 yrs. Soleus is seldom contracted in diplegia, it is more commonly contracted in hemiplegia.
Equinovarus:Commonly seen in hemiplegia. Forms (<)20% of subtalar foot problems. The deformity develops due to muscle imbalance, in which the tibialis posterior and anterior overpower the peronei. Persistent weight bearing on the lateral border of foot causes overgrowth of the base of first metatarsal. Treatment : Supple deformity - orthotics. Severe deformity - early and middle childhood; intramuscular lengthening of tibialis posterior. Adolescents : tibialis posterior split transfer to peroneus brevis. Fixed heel varus-usually due to neglected foot or failed surgery; calcaneal osteotomy. Fixed equinovarus-Triple arthrodesis/ talectomy.
Valgus:Most common in diplegia and quadriplegia. Causes : multifactorial—muscle imbalancebony malalignment, genetic predisposition & response of ligamentous structures.
Treatment:Early childhood-orlhosis.
Surgery:Indications: severe deformity-difficulty in orthotic / foot wear, pain or progressive deformity, Age : after 10 yrs. Chances of recurrence if operated at a younger age. Lateral column lengthening : osteotomy between the middle and anterior facets of os calcis, bone grafting and internal fixation. Not suitable for severe fixed valgus and hypermobile foot. Sub talar fusion; suitable for hypermobile foot and household ambulators will cause arthritis in the adjoining joints in the long term. Triple arthrodesis; used in severe deformity. The fusion should extend to medial cuneonavicular joint.
Hallus valgus:Cause; hind foot valgus. In addition to MTP joint deformity there may be growth plate disturbance in the proximal phalanx.
Treatment:Mild and supple deformity - No treatment.
Moderate:Hind foot correction, soft tissue correction,?PP osteotomy. Severe-Fusion.
23. Flat Foot
Dr. Dhiren Ganjwala
Flat foot is a common presenting complaint in the pediatric orthopedic practice. Even though it is a common finding the exact incidence of flat foot in children is unknown.
All children have only a minimal arch at birth and more than 30% of neonates have a calcaneovalgus deformity of both feet. This condition generally resolves without treatment and very rarely is corrective casting necessary.
Most children who present to an orthopedist for eduation of flat foot will have a flexible flat foot that does not require treatment. Nor have any of the various types of supports ever been shown to change the arch architecture. Although parents are often concerned about pediatric flat foot, the child is usually found to be asymptomatic, and no treatment is indicated. In most instances, the best treatment is simply taking enough time to convince the family that no treatment is necessary. Surgical management is rarely indicated for a true flexible flatfoot. A variety of tendon transfers and reconstructive procedures have been advocated, but none has proved uniformly successful.
Nevertheless, one must rule out other conditions that do require treatment, such as congenital vertical talus, tarsal coalition and Skewfoot. Untreated, congenital vertical talus may result in an awkward gait; manipulation and casting have been tried, but most authors now agree that surgical treatment is required. Although tarsal coalitions can become asymptomatic in adulthood, the anatomy will never be normal. Resection and interposition of the extensor digitorum brevis is the treatment of choice for calcaneonavicular coalitions, the results of treatment of talocalcaneal coalitions are less predictable. Skewfoot should be treated by manipulation and serial casting as soon as it is detected. In the older child, hindfoot stabilization and realignment of the midfoot may be necessary.
24. Non Operative Management of Club Foot
Dr. R. A. Agrawal, Dr. Anuj Kr. Jain
Introduction:
Agrawal Orthopaedic Hospital, Jubilee Road, Gorakhpur-273001 (U.P.), IndiaAll Idiopathic club feet are treated with preliminary serial casting. However 70-95 percent cases need Postero-Medial-Release (PMR) surgery, which leads to long-term stiffness and weakness. Ponseti group needed surgery only in 11 percent of patients.
Material and Method:150 young children (230 feet) were treated by this method. Serial casting begins within first six months of life. Abduction applied to metatarsals, counter pressure on neck of talus not calcaneus, never pronate the foot. Weekly casting for 4 to 7 weeks, Percutaneous Achilles Tenotomy under local anesthesia in 90% cases, casting for three weeks followed by foot abduction arthrosis 23 hours a day for three months and night time for three years. Only 10% need anterior tibialis tendon transfer at the age of 2½ to 4 years.
Results:
Conclusion:PMR surgery required Average Duration of casting Final Dorsiflexion Final plantar flexion Ponseti Group 4/150 (3%) 2 months 32° (10-45°) 50° (25-70°) Control Group 74/80 (94%) 3 months 8° (5-20°) 29° (10-40°) - Our study shows successful results in 150 cases.
- Simple
- Highly effective
- Less expensive (less need for hospitalization)
- Eliminates need for PMR in vast majority of patients.
- Leads to stronger, more flexible feet and better long-term outcomes.
- Based on our success, we no longer think that PMR is required for most cases of idiopathic clubfoot. Longer follow-up will determine whether we can continue to match with Ponseti's reported outcomes.
25. Restoration of Dynamic Stability of the Patella by Pes Anserinus Transportation
Prof. D. P. Baksi, M.S.,FRCS., M.S.Orth., Ph.D.Orth., FAMS, Kolkata
Introduction:Lateral instability of patella is a common clinical entity generally encountered in children. There are three clinical types : recurrent dislocation where dislocation is episodic and having no contracture of soft tissues lateral to patella, but medial stabilization appears weak : habitual dislocation of patella in flexion, where knee flexion is always associated with displacement of patella and both lateral contracture and medial laxity are present. Habitual dislocation of patella in extension is extremely rare. Permanent dislocation of patella where there is persistent lateral dislocation in an positions of knee where both the lateral contracture and medial laxity are present. This variety may be congenital due to mayodysplasia ( Stanisavaljevic, Zemenick and Miller 1976) where there is development failure of medial rotation of quadriceps or acquired as a result of progressive superolateral muscle contracture.
The object of this paper is to ensure stability of patella in the intercondylar groove in different positions of knee.
Materials and Methods:Twenty patients had 21 recurrent dislocations, 47 patients 62 habitual dislocations and 27 patients 37 permanent dislocations of patella. Ages varied from 5 to 31 years (average 11.5 years).
Methods:The surgical techniques were reported by Baksi in JBJS (Br) 1981 63 B, 399-403 and in JBJS (Br) 1993, 75 B, 305-310.
Superolateral contracture release:In habitual and permanent (acquired) dislocations the superolateral contracture release consists of the release of lateral patella-femoral capsule down to ligamentum patellae and vastus lateralis in all, rectus femoris in 65% and vastus intermedius in 62% cases are required to allow the patella to retain in the inter-condylar groove in fully flexed position of knee. In recurrent dislocation of patella these release is not indicated as there is no such contracture where only vastus medialis is weak.
Medial stabilisation of patella:This is ensured by the detached lower three quarter of Pes - Anserinus transposed to anterior surface and medial border of patella and the ligamentum patella in all types of dislocations. In congenital dislocations, lateral release with medial imbrication of vastus medialis obliques muscle ( Beaty Technique) or Pes - Anserinus transpositions to patella may be carried out.
Results:Mean followup was 15.6 years (3 to 26).The cases were evaluated by clinical, radiological electromyographical studies. Following a criteria ( Baksi 1981) the cases with recurrent dislocations showed 76.2% excellent and 23.8% good results; habitual dislocations showed 50% excellent 35.5% good, 8.3 % fair and 6.2% poor results and permanent dislocations showed 51.8% excellent and 29.6% good, 11.2% fair and 7.4% poor results. Four had recurrences among the cases with habitual and permanent dislocations during early postpositive period due to faulty operation techniques ( inadequate superolateral contracture release and wrong placement of Pes Anserinus over medial capsule), rectification of which prevented further recurrences. Quadriceps lag disappears in average 3.2 months. Retropatellar asymptomatic degenerative changes occurred in 7% cases.
Conclusion:Realignment of dislocated patella followed by Pes Anserinus transpositions being a relatively unstretchable physiological sling, provided dynamic stability of patella. This can be used reliably before epiphyseal closure and also in adults.
26. Ayurveda & Paediatric Surgery
Dr. B. B. Mishra, Ph.D.
Dallana, a commentator of the Susruta Samhita refers to three great scholars of Paediatrics- Parvataka, Jivaka and Bandhaka. Of them only Jivaka has come to us as the redactor of the present Kasyapasamhita. Besides it there are only few books on Paediatrics such as Balakumaratantra, Kumaratantra or Dasagrivabalatantra by Ravana. Balachikitsamrta by Kalyana Varma, Balatantra and Yogasudhanidhi. The Balakumaratantra by Ravana has been translated into Chinese in the 6th Cen. A. D. according to the Bibliotheca National, Paris. But only and the most important ancient Indian text on Paediatrics available to us now is the didactic Kasyapasamhita conceived and propounded by Kasyapa to Jivaka, son of Richika who abridged it at Kankhala (Haridwar). It was accidentally lost but retrieved by Anayasa yaksa, who later on passed it to Vatsya a lineal of Jivaka, the older. Vatsys re-edited the compendium in its present form, which is still older than Charaka and Susruta and is not later than sixth century B.C.
Kasyapa though a paediatrician discusses in brief surgical problems when asked by his pupils. But he is cautious that one should not discuss in detail the special branch of others than his own. If he tries to do it, he would be just like a greedy crow among intellectuals. But there is no denying the fact that the paediatrician must also have knowledge of surgery not for the sake of finding faults of surgeons but for the larger interest of children (for emergency). Therefore Kasyapa gives an outline of paediatric surgery in the chapter dvivraniya chikitsadhyaya (Treatment of two types of wounds).
According to him there are two kinds of wounds, nija or idiopathic and caused by accident or inflicted (agantu) Idiopathic wounds or sores are caused by imbalance of two or three vital elements whereas accidental wounds are of eight types : (i) fracture (Ksatabhagna), (ii) Viddha (Pierced), (iii) Patana (Lacerated), (iv) dagdha (burn) (v) Chhinna (dislocation), (vi) nispista (crushed), (vii) abhiluna (deep cut), and (Viii) caused by arms, grass, wood, fire, poison, teeth, nail, chants etc.
As far various steps in management of wounds Kasyapa holds that no wound is free from infections. Even if there is prick in the skin there is every chance of getting it infected and such wound is idiopathic while the traumatic are those which can be seen clearly. Kasyapa describes seven steps, Charaka thirty six while Susruta expands it to sixty steps of wound management. Kasyapa's seven step management are :
(i) Sansamana (fomentation or waste with lotion), (ii) Vandhana (bandage), (iii) Utklinnamansa Praksalana (Washing of protruded flesh), (iv) Kalkapranidhana (Spreading of herbal paste or medicinal powder), (v) Sodhana (dressing), (vi) Ropana (healing of wounds). (vii) Savamikarana (recolourisation of skin or area of scar).
Kasyapa advises against drainage (sravana), incision (patana), cauterization (dahana), sivana (suturing or stitching), probing with forceps (aisana) and applying force (sahasa) in case of very young baby. At another place he forbids lithotomy (removal of stones by operative measures) in children. Instead he prescribes lithorite medicine. He adds that if the wound is in vulnerable place of the child or a lactating mother surgical operation should be avoided. Instead the wound or blisters should be brushed lightly and bandaged with cow milk curd added with a little salt. Wound in other places should be properly operated. Such operation should be done only after proper examination and by competent doctor otherwise a quack will not be able to check excessive blood loss which may prove fatal as the child does not have plenty of blood.
Giving details of the procedure Kasyapa advises as the first step that if the blister is of wind origin the patient should be administered with demulcent or fatty substance and treated with gel or paste of oily base. Wounds of bile origin should be washed properly with cold water, milk, herbal paste of cool properties, etc. The wounds of phlegm origin should get hot fomentation, cauterization, hot water fomentation, bandage, drainage and the patient should be put to fast.
The second step is to properly bandage the wound. Kasyapa holds that it should he done with properly washed old cloths in such a way as the applied medicines do not fall away and at the same time is not very painful to the child. If the bandage is stiff, it will result in sore, inflammation, burning sensation, fever and thirst and if it is loose, medicine applied will not be in proper place. Therefore it is advised to be neither stiff nor too loose. The purpose of bandage is said to protect the wound against infection caused by air pollution, sunshine, grass, wood, water, houseflies, etc. But bandage should not be applied on wounds with febrile condition, with burning sensation and with living pathogens or in erysipelatis (Visarpa). It is laid down that wounds of bile origin should be washed or dressing done twice daily. For antiseptic and healing purposes powder of turmeric (haldi), daruhaldi, seasamum (tila), ghee, rocksalt, mulahatti, trivrtta, honey and powder of margarossa leaf (Neem) should be sprinkled. It is to be noted that recent researches have proven the efficacy of Neem leaves as very antiseptic, while powder of daruhaldi has anti-inflammatory and analgesic properties. Rock salt, ghee, honey, etc. are best of known for healing purposes. Spreading of herbal paste and dusting of wounds with herbal medicines hastens healing.
Post-operative management by Kasyapa is not available to us as the only hand written palm leaf manuscript of his work is damaged. But there is no doubt about its existence in the original copy because the last but not the least stage of treatment has survived the damage. Prescriptions have been provided for re-pigmentation (savarnikarana) of the skin to its natural colour and helping in the growth of hair follicles (lomotpadana) on the scar left by the wound or surgical operation. Now-a-days no much attention is devoted by paediatric surgeons or even general surgeons to these procedures. They are recommended and done separately by plastic surgeons for cosmetic purposes only. Kasyapa along with Charaka & Susruta have discussed different herbal pastes for re-pigmentation of the skin. As for the growth of hair follicles on the scar Kasyapa advises spreading of oil on the skin and dusting it with the ashes of skin, hair, horn, hoof and bones of four footed animals. The same verse has been reproduced by Charaka and Susruta which again proves the antiquity of Kasyapasamhita to two other compendiums. The efficacy of these medicaments needs clinical trial.
As for idiopathic ulcers, Kasyapa divides them into eight, Charaka—seven and Susruta into ten types. Among the eight types of ulcers three belong to phlegm type, three to bile, one to wind and one due to imbalance of all three vital elements. Their detailed clinical features have been provided and is advised to be treated like other wounds. Even surgical knife is recommended if it is red and pus has formed. In some cases cauterization is to be done. Kasyapa further adds that children who are very active, walk to and fro very briskly and even run are prone to bruises and injury caused by grass, wood, brick, arms, etc. which may give acute pain. Such cuts and bruises should be properly washed and given hot water fomentation but if it is bleeding, cold water should be applied. So these bruises should be treated first with fomentation, followed by cauterization, Ksarakarma and then bandaged with honey and ghee so that it may heal up in due time.
Ayurveda lays utmost importance upon diet and life style of a man. Any improper vitiation will cause ample harm and disease. Kasyapa opines that good health is dependent on diet and there is no medicine like it. Any disease can be cured by proper diet. Without food, no body can survive only on medicine and that is why diet has been rightly termed as the greatest medicine or mahabhaisjya. So diets suitable to the age, constitution of the body, temperament, taste of the person, and keeping in view the season and country in question should be prescribed for the patient. A detailed guideline had been provided and emphasis has been laid on proper diet, life style and proper physical exercise by Kasyapa (Yuktahara viharasya yuktavyayamasevinah). If they are followed properly one would keep oneself free from diseases. Use of garlic and milk have been highly recommended by him in fracture, dislocation of bones and other bone diseases.
Conclusion:we find that from very early days of human existence man tried to grapple with all the problems encountered by him including health. Necessity is the mother of invention, so new and newer methods of diagnosis, medicaments, methods of rehabilitation, etc. were discovered to alleviate or assuage pangs of physical and mental afflictions. India was a fore runner and pioneer in this field. The ancient compendiums on Ayurvedic medicine and surgery are beckon light even today for millions of people here. The only need of the hour is to reinterpret it in modern scientific terminology, network of laboratories and extensive field trials of herbal medicines which are not only free from adverse side effects and reactions of modern day drugs but are though slow but effective in long term. However, the day to day progress of far reaching consequences in the field of modern medicine and surgery have to be properly evaluated and amalgamated to make Ayurveda, more effective and acceptable to the mass.