Abstracts
1. Orthopedic Manifestations of Pseudoachondroplasia
Hae-Ryong Song, M.D., Korea
This study included 11 patients, aged from 3 years to 44 years (average 22 years), with a diagnosis of PSACH. There were four meals and seven females. Three patients were young children. Four patients in two families included two mothers and two sons.
The average height of patients older than 17 years (eight patients) was 113.7 cm. The average ratio of trunk height to limb height in 11 patients was 1.47 (normal ratio [NR] ? 0.95) and the average ratio of arm span to height was is 0.96 (NR?: 1.00). These results demonstrated that pseudoachondroplasia had short-limb dwarfism. The average ratios of radius length to humerus length and tibia length to femur length were 0.69 (NR=0.75) and 0.77 (NR=0.82), respectively. In upper extremity of 11 patients, there were one rhizomelic shortening and 10 mesomelic. However, whereas in lower extremity, there were four rhizomelic and seven mesomelic. All patients showed the normal intelligence, nearly normal head and face. The fingers and toes were short and thick. The hips in three children showed delayed ossification of the femoral epiphysis, widening of the tri-radiate cartilage and the ischiopubic junction, and decreased thickness of the femoral physis. The adult hip showed varus deformity of the proximal femur, short neck overgrowth of the greater trochanter, acetabular dysplasia, lateral subluxation, and premature osteoarthritic changes. Two patients had osteochondritis dissecans at the femoral head. The mechanical alignment of lower extremity showed varus deformity with the average MAD, ranging from 39mm to 64mm in 10 patients. One patient, who was a wheelchair-bound ambulator, had windswept deformity. In coronal plane, the proximal tibia had varus deformity in 10 patients and valgus deformity in one patient. The distal femur had varus in nine patients and valgus in two. The distal tibia had varus in five, valgus in four, and neutral in two. In three children, the epiphyses of long bone showed narrow physis and small epiphysis within widened metaphysis like ball-in-socket in children. In the sagittal plane, the distal femur had procurvatum deformity in all patients. The proximal tibia and the distal tibia had procurvatum or recurvatum deformity.
Ligament laxity was shown in all joints except the elbow. All patients had flexion contracture of the elbow with varying severity. The flexion contracture was related to posterior bowing of the proximal ulna and the distal humerus. The deltoid tuberosity of the humerus was prominent in all patients. Nine patients showed that the wrist had Madelung-like deformity combined with ligament laxity. The knee joint showed severe ligament laxity than the other joints.
The knee had multidirectional instability, and the laxity of the MCL was more severe than those of ACL, LCL, and PCL. Three adult patients (27%) showed C1-C2 joint instability associated with os odentoideum rather than hypoplasia of dens. The sagittal images of CT scan during flexion and extension of cervical spine demonstrated that the space between os odontoideum and atlas was not changed. However, SAC decreased about 50% during flexion compared to that during extension because the upper part of dens moved posteriorly during flexion. One patient had incomplete reduction at the non-union site between the os odontoideum and the dens during extension. He had compression myelopathy due to basilar impression and severe compression of spinal cord in CT scan and MRI. This patient also had compression of spinal cord at the upper lumbar spinal cord in MRI. He underwent decompressive surgery and posterior fusion of C1-C2 joint with extended position. He showed decreased length of the pediclecle at the lower lumbar spine in lateral view of radiograph. The other two patients with complete reduction had no myelopathy.
References:- Briggs MD, Chapman KL. Pseudoachondroplasia and multiple epiphyseal dysplasia: Mutation review, molecular interactions, and genotype to phenotype correlations. Hum Mutat 2002;19:465-78.
- Briggs MD, Hoffman SM, King LM, et al. Pseudoachondroplasia and multiple epiphyseal dysplasia due to mutations in the cartilage oligomeric matrix protein gene. Nat Genet 1995;10(3):330-6.
- Ferguson HL, Deere M, Evans R, et al. Mosaicism in pseudoachondroplasia. Am J Med Genet 1997;70:287-91
- Ford N, Silverman FN, Kozlowski K, et al. Spondyloepiphyseal dysplasia (pseudoachondroplastic type). Am J Roentgenol 1961;86;462.
- Herring JA. Tachdjian? Pediatric Orthopaedics 3d ed. Philadelphia: W.B. Saunders 2002:1523-1527
- Horton WA, Hall JG, Scott CI, et al. Growth curves for height for diastrophic dysphasia, spondyloepiphyseal dysphasia congenital, and pseudoachondroplasia. Am J Dis Child 1982;136:316-9.
- Hunter AGW. Perceptions of the outcome of orthopedic surgery in patients with chondrodysplasia. Clin Genet 1999;56:434-40.
- Kopits SE. Orthopedic complications of dwarfism. Clin Orthop 1976;114:153-79.
- Manabe N, Nakamura K, Ikegawa S. Kimizuka M. A mild form of pseudoachondroplasia: minimal epi-metaphyseal involvement of long bones. Eur J Radiology 1998;28:155-159.
- Maroteaux P, Stanescu V, Les formes pseudo-achondroplasiques des dysplasies spondylo-epiphysaires. Press Med 1959;67:383-6.
- Maroteaux P, Stanescu V, Fontaine G. The mild form of pseudoachondroplasia. Eur J Pediatr1980;133:227-31.
- Mckeand J, Rotta J, Hecht JT, Natural history of pseudoachondroplasia. Am J Med Genet. 1996;63;406-10.
- Mortier GR. The diagnosis of skeletal dysplasias: a multidisciplinary approach. Eur J Radiol 2001;40:161-7.
- Nakajima K, Onomura T, Tanida Y, et al. Factors related to the severity of myelopathy in atlantoaxial instability. Spine 1996;21:1440-5
- Nash CL, Moe JH. A study of vertebral rotation. J Bone Joint Sur 1969;51A:223.
- Paley D. Principles of Deformity Correction. 1st ed. Berlin, Springer-Verlag, 2002:; 19-30.
- Stanescu R, Stanescu V, Muriel MP, et al. Multiple epiphyseal dysplasia, Fairbank type. Morphologic and biochemical study of cartilage. Am J Med Genet 1993;45(4):501-7.
- Stanescu V, Maroteaux P, Stanescu R. The biochemical defect of pseudoachondroplasia. Eur J Pediatr 1982;138:221-5.
- Svensson O, Aaro S. Cervical instability in skeletal dysplasia. Report of 6 surgically fused cases. Acta Orthop Scand 1988;59(1):66-70.
- Unger S, Hecht JT, Pseudoachondroplasia and multiple Epiphyseal dysplasia: New etiologic developments, Am J Med Genet 2001;106:244-250.
- Watanabe M, Toyama Y, Fujimura Y. Atlantoaxial instability in os odontoideum with myelopathy. Spine 1996;21:1435-9.
- Wynne-Davies R, Hall CM, Young ID. Pseudoachondroplasia: clinical Pseudoachondroplasia: clinical diagnosis at different ages and comparisons of autosomal dominant and recessive types. A review of 32 patients (26 kindreds). J Med Genet 1986;23:425-34.
2. Is Scoliosis Ideopathic?
Dr. Arun Goel
Mool Chand KR Hospital
B-114, Swasthya Vihar
Vikar Marg, Delhi – 110 092
From time immemorial many conditions were labeled as idiopathic and gradually with time and understanding of the problem, people have been able to explain the aetiological basis.
In view of that it was felt to look in greater details of the Idiopathic Scoliosis group. A survey & retrospective study was carried out of all the cases of scoliosis treated in the last 20 years (1954-1974) at Robert Jones Agnes Hunt Orthopaedic Hospital, Oswestry, U.K., University of Liverpool. New cases were also studied in the year 1975-1981 at MAMC and LHMC. The number of cases studied were 187 at Oswestry and 43 at New Delhi. It was observed that 60% of cases labeled as Idiopathic had associated problems: Café-au-lait spots, plagiocephaly, asymmetry in leg length, a family history of scoliosis, menstrual disorders, eye and mental changes. This probably leads one to think that so called Idiopathic Scoliosis is not idiopathic but dysplastic. Details regarding various associated anomalies and their significance as a possible aetiological factor in causation of scoliosis will be discussed.
3. Certain Random thoughts on Research in Health Care
Dr. Jayaprakash Muliyil, MD, Dr. PH
Epidemiology provides the logical basis for health care, be it in the process of diagnosis, choice of interventions or in assigning causal connections. The expression “evidence based medicine” appears to suggest that there is a kind of medicine being practiced which is not quite evidence based. It is imperative that we constantly re-examine our practices and beliefs so that unscientific elements are weeded out in the light of accumulating information. Research essentially involves an inquiring frame of mind, which transforms information into theories as to how things actually work. Information by itself is of little value unless it is viewed in the context of a theory. Scientific inquiry progresses in a hypothetico-deductive fashion where empirical evidence is gathered to falsifying theoretical constructs. In the absence of evidence to the contrary our theories shall prevail. Statistics help us essentially in the following 3 areas.
- Measurement of various parameters precisely.
- Adjusting for confounders
- Measurement of interaction
By and large most errors that creep into our research initiatives are non-statistical in nature. Hence the process of gathering information, whether primary or secondary, attains paramount importance in allowing us to make valid conclusions. The paper will attempt to highlight certain important issues related to study designs analysis and interpretation.
4. Ultrasonographic Technique for the Diagnosis of DDH
Nobuyasu Ochiai, Makoto Kmegaya, Takashi Saisu
Chiba Children’s Hospital, Division of Orthopaedic Surgery, Japan.
It is sometimes difficult to diagnose DDH, especially in a newborn child using a radiological exam. In the past, we had to rely on a physical examination, such as Ortlani or Barlow’s test. Ultrasonographic technique is very useful and safe procedure for DDH children. Graf (1980) described an ultrasonographic technique for the diagnosis of congenital dislocation and subluxation of the hip. Following this, ultrasound has become more prevalent in diagnosing as DDH.
Graf technique:Method: When we perform this technique, it is useful to use a special table invented by Graf, and set the baby in the lateral position. The machine we used was Toshiba SSA-100 A, 7.5 MHz (occasionally 3.75MHz) linear-type scanner. The scanner must be longitudinally and vertically against the long axis of the body and set just above the greater trochanter. At first, we must seek the distal end of the iliac bone and also detect a straight line of the iliac bone, which is horizontal on the monitor. The scanner is adjusted until we can get the proper image. Once we can get the image and fibrocartilaginous limbus, we print it out.
Classification and measuring:
For the next step, we draw three major lines on the image as follows:
a) Base Line: This is the line, which connects the bony promontory, and the point that the membrane of the cartilage roof connects to the iliac bone.
b) Bony roof line: This is the line which connects the bony promontory and distal end of the iliac bone.
c) Cartilage roof line: This is the line which connects the bony promontory and the center of fibrocartilaginous limbus.
For the next, measuring a and ß angle. Based on these two angles, we classify into four groups.
a angle : the angle which is made by the base line and the bony roof line.
ß angle : the angle which is made by the base line and the cartilage roof line.
Type 1a : a angle > 60 degree, ß angle < 55 degree
1b : a angle > 60 degree, ß angle > 55 degree
Type 2a : a angle = 50 ~59 degree, ß angle > 55 degree (under 3 month year old)
2b : a angle = 50 ~59 degree, ß angle > 55 degree (over 3 month year old)
2c : a angle = 43 ~49 degree, ß angle < 77 degree
2d : a angle = 43 ~49 degree, ß angle >77 degree
Type 3a : a angle < 43 degree, ß angle > 77 degree (nothing in the cartilage roof)
3b : a angle < 43 degree, ß angle >77 degree (high echo area in the cartilage roof)
Type 4 : high dislocation, a angle < 43 degree, ß angle >77 degree
Purpose: Diagnosis of the DDH in the abduction position and recognition of the reduction position while treating by plaster cast and Pavlik Harness.
Method:Set the baby in a plaster cast or Pavlik harness in the supine position. We put a linear scanner on the hip perpendicular and transversal to the long body axis. The guideline for the proper scanning level shows the delineation of the public tubercles and the medial aspect of the femoral metaphysis. The machine we used was a Toshiba SSA-100 A, 3.75 MHz (occasionally 7.5 MHz) linear-type scanner. This is better than a sector type for revealing anatomical relationships. Each hip is scanned separately. On the monitor, the two distances are measured to describe the position of the femoral head quantitatively. First of all, X and Y axes are identified on the monitor. The X axis is a line connecting the two peaks of the public tubercles; Y axis is a line that passes at a mid point of the two peaks of the public tubercles, perpendicular to the X axis. The cross point of the two axes becomes the origin. One, the X value is the distance between the most supero-medical point of the proximal femoral metaphysis and the Y axis. The X value defines lateralization of the femoral head. Secondly, Y value is the distance between the most supero-medial point of the proximal femoral metaphysis and the X axis. The Y value defines the degree of the depth of the femoral head. The two distances are delineated and easily measured on the monitor. The scanning is also done on the unaffected sides.
Position of the normal and dislocated femoral head:a) Normal side: We can recognize the shape of the femoral head in the acetabular socket. The adductor muscle and joint capsule lie horizontally over the femoral head. We can recognize the ossific center when it appears. The femoral head is situated at the point X value: average 37.9mm and the point Y value average 7.2mm.
b) Dislocated side: We cannot recognize the femoral head in contrastive position to the normal side. If the baby is DDH, there is nothing in the acetabular socket and adductor muscles head askew to the latero-inferior direction. The position of the dislocated femoral head is situated in a more lateral and deeper position. If abduction is severely restricted, we cannot find the femoral head easily. However, it is possible to find it by tracing the femoral shaft successively.
5. Acetabular Development after Reduction in DHH
Sharaf Ibrahim
Department of Orthopaedics and Traumatology, Faculty of Medicine,
University Kebangsaan Malaysia, Kuala Lumpur
The triradiate cartilage of the acetabulum contributes 70% to acetabular growth, enlarging both the diameter and the depth. The acetabular ring apophysis contributes 30% to acetabular development by deepening its lateral aspect. It contains the secondary ossific nuclei, which start to ossify in early lie and fuses completely to form the definitive acetabular margin later in adolescence The fibrocartilaginous labrum further deepens the acetabulum. The concavity of the acetabulum develops in response to the presence of the femoral head (Portinaro et al 2001).
In infants with DDH, the degree of acetabular dysplasia at birth ranges from mild to severe. Important factors for normal acetabular development are the age of the patient at the time of reduction and the concentricity of reduction. Wientroub et al (1979) showed a good response to closed reduction and cast immobilization in infants between 3 and 6 months of age with CDH. Even after the age of 5 years there was continued improvement in the development of the acetabulum.
There is controversy regarding acetabular remodeling in the child after the age of 18 months. Both Salter (1961) and Pemberton (1965) felt that little correction would occur with femoral head reduction alone after 18 months of age. However, others (Harris et al 1975 and Brougham et al 1988) have found that acetabular correction will occur following closed or open reduction up to 4-5 years of age.
Kasser et al (1985) performed proximal femoral varus derotation osteotomy to treat persistent acetabular dysplasia in CDH. Good results were obtained in patients less than 4 years of age at the time of surgery. Four out of 13 patients between 4 and 8 years of age showed persistent dysplasia and there was no benefit in 10 out of 11 hips in patients older than 8 years. Acetabular growth following pelvic osteotomy is well maintained. In most studies, the acetabular angle decreases further towards the end of growth (as ossification of the lateral acetabular apophyseal centres occurs). (Fritsch et al 1996).
References:- Brougham DI, Broughton NS, Cole WG, Menelaus MB. The predictability of acetabular development after closed reduction for CDH. J Bone Joint Surg 1988; 70B:733-36
- Fritsch EW, Schmitt E, Mittelmeier H. Radiographic course after acetabuloplasty and femoral osteotomy in hip dysplasia. Clin Orthop 1996; 323:215-25.
- Harris NH, Llyod-Roberts GC, Gallien R. Acetabular development in CDH. J Bone Joint Surg 1975; 57B:46-52.
- Kasser JR, Brown JR, MacEwen GD. Varus derotation osteotomy in the treatment of persistent dysplasia of the hip in congenital dislocation of the hip. J Bone Joint Surg 1985; 67A:195-202.
- Pemberton PA. Pericapsular osteotomy of the ilium for the treatment of congenital dislocation and subluxation of the hip. J Bone Joint Surg 1965; 47A:65-86.
- Portinaro NM, Murray DW and Benson MKD. Microanatomy of the acetabular cavity and its relation to growth. J Bone Joint Surg [Br] 2001; 83B:377-83.
- Salter RB. Innominate osteotomy in the treatment of congenital dislocation and subluxation of the hip. J Bone Joint Surg 1961;43B:518-39
- Wientroub S, Green I, Terdiman R and Weissman SL. Growth and development of congenitally dislocated hips reduced in early infancy. J Bone Joint Surg 1979; 61A:125-30
6. Effects of Shock Waves on Immature Rabbit Acetabulum
Possibility of noninvasive treatment for residual acetabular dysplasia after DDH
Takashi Saisu, Makoto Kamegaya, Nobuyasu Ochiai, Kenji Takahashi, Shigeru Mitsuhashi, Yuichi Wada, Hideshige Moriya,
Division of Orthopaedic Surgery, Chiba Children’s Hospital and Department of Orthopaedic Surgery, School of Medicine, Chiba University, Chiba City, Japan
We conducted this study using immature rabbits to verify whether or not bones formation is induced by irradiation of extracorporeal shock waves on acetabular roof, and our final goal is to apply the extracorporeal shock waves to the clinical practice for the treatment of residual acetabular dysplasia after DDH.
Method:Eight male New Zealand White rabbits aged 9 weeks were used. Piezolith 2300 (Richard Wolf Inc., Germany) was used to produce extracorporeal shock waves. Ultrasonic waves were used for focusing. The focus was set in 3 mm cranial from superolateral edge of the acetabulum and 2mm inside from lateral margin of the acetabular roof. Each 4 animals of the 8 animals were grouped into Group I and II. Shock waves were irradiated on the right acetabular roof from outside. The strength and the number of the shock wave were set to be 100 MPa and 5000 times respectively. The animals were monitored for 4 weeks in group I, and for 8 weeks in group II. After the monitoring period, the pelvises were embedded in polyester resin and were cut into 1 mm serial sections (0.3mm in width) which were parallel to the plane including the center of the body of the last lumbar vertebra and bilateral acetabular fossa. Contact microradiograph of each section was taken, and the section that has the widest microradiograph of this section, the distance “y” (the breadth of the acetabular roof) was determined and the laterality was examined. Line a was drawn from left to right superolateral ossified edge of the acetabulum, and then Line “b1” and “b2” were drawn perpendicular to the Line “a” from bilateral medial margin of the acetabulum. The distance from line b1 or b2 to the lateral margin of the acetabular roof at “x” (0-8) mm cranial from line “a” was determined as “y”. Statistical analysis was conducted using the unexposed side as control by Student’s paired t-test.
Results:No fracture was observed on the plain X-ray photo during the monitoring period after irradiation. Four weeks after irradiation, the breadth of the acetabular roof in exposed side was significantly increased at (“x”=) 1, 3 and 4mm cranial area from the line “a”. Eight weeks after irradiation, the breadth of the acetabular roof in exposed side was significantly increased at (“x”=) 4, 5 and 6 mm cranial area. On the contact microradiographs of the acetabular roof 4 weeks after irradiation, new bone formation was markedly observed on the lateral margin of the acetabular roof in exposed side.
Discussion:This study was intended to induce bone formation at the area, which has no requirements of covering in biomechanically, and the extension of cartilage coverage in the hip joint was out of this scope. As shown in these results, new bone formation on the acetabular roof and significant increase in the breadth of the acetabular roof suggested that there would be a possibility to use extracorporeal shock wave therapy for the treatment of acetabular dysplasia. The number of test subjects was not sufficient to conduct a statistical analysis, but histological changes were observed markedly. We supposed the area of new bone 4 weeks after irradiation moved to carnial side accompanying with the bone growth in the proliferation zone in the acetabular roof and the breadth of the acetabular roof at cranial area increased as a result of that. In conclusion, irradiation of the extracorporeal shock wave induced acetabular augmentation. The clinical application of the extracorporeal shock wave is still far from its actualization. This report is the first step to actualize the non-operative acetabuloplasty.
7. Microsurgery in Paediatric Orthopaedics
Dr S Raja Sabapathy MS M Ch DNB FRCS (Edin)
Head, Department of Plastic Surgery, Hand Surgery and
Reconstructive Microsurgery Ganga Hospital, Coimbatore
Microsurgery is the marvel of Modern surgery. It dramatically improved the surgeon’s capability. Reattachment of amputated parts became possible, and the results of many frequently done procedures improved. Practice of this fine technology is more demanding in children, but when successful better results are achieved than adults. Three areas where Microsurgery is mainly useful in Orthopaedics are;
1. Replantation of Amputated Parts
2. Free tissue transfer
3. Nerve repair
The first documented replantation was in the Paediatric age group. Malt replanted the arm of a 12 year old boy in Boston in 1962. Popularly called as the ‘Boston arm’, it heralded a new era in trauma care. Replantation in children is more difficult because of the small caliber and delicate nature of the vessels. The survival rate of replants in children is lower than adults, usually between 60 to 70% (1). But it not impossible and most reputed units successfully replant up to the distal interphalangeal joint of fingers on a regular basis. If paediatric replantation is successful, the result function is better than adults.
Enhanced ability for nerve regeneration, tendon gliding and bone healing and joint motion promotes a superior return of sensory and motor capacities in children. Maintenance of growth after replantation is a major concern. A successful replantation of limb or digit in children must allow for epiphyseal growth to skeletal maturity. Most studies show that replanted digits show 80-90% of growth of the uninjured extremity. This is also reflected in our experience. (2) The involved segment may show minor decrease in growth due to growth plate injury, but the distal segments maintain normal growth. Few reports show overgrowth in the replanted part. In children, replantation of every upper extremity amputation is considered unless life threatening factors exist. Long ischemia time, amputations at thoraco-humeral level and associated Brachial Plexus injury are the absolute contra-indications for replantation. In all other cases, serious considerations should be given to replantation of amputated parts of children. Sometimes part of the amputated part may be used either to lengthen the stump or to gain better function in what is called ‘surgical opportunism’.
Transportation ProtocolInjured Hand: Apply saline-moistened sponges to the wound and cover with a sterile, bulky dressing. If extensive bleeding is note, apply a pressure dressing rather than a tourniquet. Truly uncontrollable bleeding is rare and it must be treated surgically before transport. Splint and elevate the injured part. Check for any life threatening injuries. If not, please rush the patient to the replantation center.
Amputated Part: Please send all parts. Although all tissues may not be Replantable, various portions may be used to reconstruct missing elements. No minimal cleansing is necessary at this time. More extensive debridement is necessary prior to replantation and it will be done in the operating room. Time is not to be wasted in cleaning the part or investigating the patient. Wrap the amputated part in gauze and place it in a dry plastic bag. Place it in a box or bag containing ice. Public awareness of the possibility of replantation and the centers performing such surgeries must be increased. Most successful major replants, which we did, are the ones where the patient directly came from the scene of the accident. Some times replantation has been possible, just because of the delay at the primary center in investigating the patient even when life-threatening injuries did not exist. This has to be avoided.
Free Tissue Transfers in Children: Free tissue transfers are a valuable methodof reconstruction of defects in all areas of the body. It is quite safe in children. Unlike replantation, in free flaps success rates are comparable to that of adults. (3) When used in children they can reduce the number of stages and hospitalization days greatly reducing psychological trauma in children. One stage reconstruction can also avoid the temporary disfigurements of tissue expansion and pedicle flaps which appear unforgettably bizarre to some children. In addition to these benefits, micro vascular surgery in children can transfer growth (e.g. joint transfers) in a way conventional grafts cannot. Micro vascular surgery also extends the choice of donor sites, so that donor site morbidity can be minimized to the happiness of both the child and the parents.
Commonly Used Indication - Trauma: Defects in the lower limb sustained due to road traffic accidents is the commonest indication for the usage of free flaps in our country. When children are knocked down by vehicles and the lower limb gets caught, defects usually occur on the dorsum of the foot or along with the fracture of the both bones of the leg. Usage of free flaps in such circumstances is many times limb saving and cost effective also. Free flaps can be used in the upper extremity and results are much better in the upper limb than lower limb. Apart from cover it can be used to transfer power when muscles are neurotised in the recipient bed. This is particularly valuable in the management of Volkmann’s ischemic contracture.
Toe and joint Transfers in Children: Children are candidates for toe transfer both for traumatic loss and congenital loss. Osteoplastic reconstruction of thumb is not acceptable in children because they don’t have the growing potential. Digital joints play an important role in the growth and development of the child. The absence, abnormal function or destruction of one of these joints due to trauma, infection or disease will compromise the development, growth and function of the hand. Non vascularized joints had a high failure rate due to invasion of joint space with fibrous tissue, joint-space narrowing and cartilage degeneration. In children, vascularized joint transfer maintains growth potential, preserves joint architecture, restores joint stability and allows function in the hand. This stimulates complete, global growth.
Vascularized Bone Transfers in Children: Free vascularized Fibula is a good source of viable bone available for transfer. In children we have used it often in the management of Congenital Pseudoarthrosis of Tibia. Results have been quite good and predictable that Vascularized Fibula is the first choice when we see a child with Congenital Pseudoarthrosis. In a series of 4 children treated with Free Fibula and 5 treated with Ilizarov we found that all children treated with Free Fibula united. One child who did not unite with Ilizarov subsequently united after Free Fibula Transfer. Free fibula took 10 to 14 weeks to unite compared to 22-26 weeks for bone union with Ilizarov. Children with Free fibula have fixators for 4 to 5 months compared to 6 to 8 months of fixators in the Ilizarov technique. Further Microsurgical procedure is a single staged procedure compared to Ilizrov where these required 6 to 8 procedures on an average.
Never Surgery:Peripheral Nerve Injuries in Children: Use of magnification for never repair has given superior results. Children show better functional results than adults. Although children have better functional results clinically there is no definitive study demonstrating such superior results in children. Atraumatic microsurgical technique and principles of nerve healing are important in both age groups. However, the superior results in the paediatric age group most likely represent the child’s superior cortical adaptability and relearning capacity compared with the adult’s whose brain is relatively fixed. Postoperative immobilization is far more extensive in the paediatric patient than in the adult.
Brachial Plexus Injury: Management of traumatic brachial plexus injury runs on the same principles as that of the adults. Obstetric Brachial Plexus palsy presents a unique situation, where controversies to the treatment pathway still exist. Around 80% of the children recover fully with conservative management. It is in the small proportion we look for pointers as to who would benefit from surgery and the time frame as to when it should be offered. On the basis of the thesis undertaken by Tassin, Gilbert and Tassin proposed that failure of any recovery in the biceps at 3 months would be associated with such a poor functional recovery that nerve surgery is indicated. This is widely accepted though many authors have come up with more exhaustive protocols based on the recovery status of various muscle groups. Gilbert’s advice could be used as a guideline for clinical practice. Unfortunately direct nerve surgery is indicated. This is widely accepted though many authors have come up with more exhaustive protocols based on the recovery status of various muscle groups. Gilbert’s advice could be used as a guideline for clinical practice. Unfortunately direct nerve surgery has not become popular as much as it should be. It is still inhibited by lack of awareness of the possibilities of operative treatment and by unjustified optimism about the outcome for natural process.
Conclusion: Micro vascular surgery can offer dramatic results and improve the quality of life of many Paediatric Orthopaedic patients. Not all surgical units have the facility for this technique and although, inexperienced hands, the surgical success rate for micro vascular surgery in children is no lower than for adults, there are specific behavioural, organizational, and technical difficulties that must be addressed if this important surgery is to succeed. Every unit that practices Microsurgery should seek every opportunity to optimize the success rate of surgery. Orthopaedic surgeons should consider referring and embracing this very valuable surgical discipline, which can be so powerful when employed adequately.
References:- Baker GL, Kleinert JM, Digit replantation in infants and young children: determinants of survival. Plast. Reconstruct Surg. 1994; 94:139-145
- Raja Sabapathy S Replantation of First and Second toes – a worthwhile effort
- Kay S, Coady M. The role of Microsurgery and Free Tissue transfer in the reconstruction of the paediatric upper extremity. Ann. Acad. Med Singapore. 1995; 24: 113-23
- Kay S, Lees VC. Free tissue transfers in Children. In Growing Hand ed. Gupta A, Kay S and Scheker LR. Mosby. London 2000.p.969-986
8. Elastic Stable Intramedullary Nail Fixation of Paediatric Femoral Fractures
Unni G. Narayanan
The Hospital for Sick Children, Toronto, Canada.
Paediatric femoral fractures are treated by a variety of methods. These include various types of traction, immediate spica cast, traction followed by spica cast, internal fixation with plate and screws, external fixation, and intramedullary fixation. Orthopaedic surgeons remain divided about the optimal method of treatment for children’s femoral fractures. The choice of treatment may be influenced by the age of the child, the level and pattern of the fracture, and to a great extent by regional, institutional or surgeon’s preferences.1 A systematic review of the literature of the treatment methods of paediatric femoral fractures provides little evidence to support one method of treatment over another .2 In general, outcomes tend to be uniformly good irrespective of the method of treatment.
Elastic Stable Intramedullary Nailing:Elastic stable intramedullary nailing has become a popular method of fixation of paediatric femoral fractures. This technique, which was adapted from existing flexible rod systems was first described by surgeons from the Children’s hospital in Nancy, France 3,4. Ligier et al reported the result of the Nancy experience5. Others have also reported excellent clinical results with this technique, which has been variously called “elastic stable intramedullary nail” fixation, “flexible intramedullary nail” fixation or “Nancy nail” fixation6,9. Perceived advantages of this technique include earlier mobilization and return to function than non-operative techniques, and less disruption and smaller scars than with other surgical methods.
Biomechanical Principles:The selected straight rod is first curved (plastically deformed). During insertion the relatively straight medullary canal (compared with the contoured nail) forces the curved flexible nail to straighten within the bone. This elastic deformation creates a bending moment within the long bone, which will force the fracture to angulate in the direction and the plane of the concavity of the curved nail, as the nail wants to return to its curved state. A second nail of matched diameter and curve, which balances the first nail with an equal but opposite moment, counteracts this moment. The two intramedullary nails act complimentarily to stabilize the fracture. The fixation is not rigid but sufficiently stable that no additional external immobilization is required if performed correctly for the appropriate indication. However, any significant imbalance in the magnitude or the direction of the moment created by the two nails will result in angulation of the fracture in the direction of the stronger nail. Hence the importance of using nails of the same diameter, contouring them to same extent and inserting them so that the curves of both nails are lie in the same plane.
The titanium nails have been distinguished from other flexible nail systems such as Ender nails, made of stainless steel. The latter are believed to be insufficiently elastic for children’s fractures and, therefore have a tendency to straighten the normal bony curvature5. Sometimes 3 or more flexible rods are inserted in order to better fill the medullary canal to enhance cortical contact, and provide more stable fixation, the same principle underlying rigid intramedullary rod fixation, but not that of the Nancy nailing technique.
The chondrogenic potential of stem cells had been validated in experimental studies whereby lesion of osteochondritis dissican and physeal arrest were repaired with transplantation of MSCs.
Ideal Indications:Mid-diaphyseal transverse, short oblique or short spiral fractures of the femur with less than 25% comminution, in children from 5 to 12 years old. The use of flexible nails can be extended to more proximal including sub-trochanteric fractures and some multi-fragmentary fractures by modifying the technique to take advantage of the principles outlined above and employing some additional precautions.
Preoperative Planning:The selection of the appropriate diameter of the flexible nails is based on the estimation of the narrowest diameter of the medullary canal from the radiographs. The isthmus is typically at the junction of the proximal and middle one-third of the femur and is narrowest in the coronal plane (AP view). A pair of matched nails of the maximum diameter that can be accommodated within the canal is chosen, usually no more than 40% of the narrowest width of the canal.
Positioning:The patient is positioned supine on a standard radiolucent table. The image intensifier is positioned at right angles to the long axis of the table and is brought in from the lateral side. The c-arm should be able to arc freely below the table in order to obtain lateral images. The ipsilateral hip is flexed approximately 30 degrees with a radiolucent support under the thigh (e.g. a bolster covered with sterile towels). This raises the thigh on fractured side above the contralateral thigh to provide an unobstructed lateral view of the fractured femur. It also elevates the posterior sag, which typically occurs at the fracture site. A bump is also placed under the pelvis on the fractured side. This will raise the hip on that side so that a proximal lateral image will be able to distinguish the femoral neck of the fractured side (more anterior) from the contralateral side. It is critical that the entire femur from the hip to the knee can be imagined clearly both in the antero-posterior and lateral projections. This is confirmed prior to prepping and draping the patient. Alternatively, a fracture table may be used which makes imaging more facile but ideally requires a preoperative reduction.
Contouring the Nail:The two nails are contoured either by hand, or by a rod/plate bending device to produce a uniform bow with the nail tip pointing towards (and in the plane of) the concavity. The apex of the bow should be created at the level of the fracture so that the nail is shaped for mid-shaft fractures or shaped like an inverted comma for more proximal fractures. At the apex of the bow, the lateral (perpendicular) displacement from the original straight position is about 3 to 4 times the width of the medullary canal at the fracture site. The bow in each nail should be matched.
Insertion Technique:The nails are inserted in a retrograde fashion from the medical and lateral sides respectively. Under the image intensifier the level of the distal femoral physis is demarcated on the skin. The incisions are mid-lateral and mid-medial respectively, measuring 3.0 cms, oriented longitudinally, and centred over the physeal line. On the lateral side the iliotibial band is incised in line with the skin incision. The vastus lateralis fascia is divided and vastus lateralis muscle is retracted anteriorly off the intermuscular septum to expose the periosteal surface of the lateral supracondylar flare of the distal femur. On the medial side the deep fascia is divided to expose the distal margin of the vastus medialis obliqus which is retracted anteriorly to expose the periosteal surface of the medial supracondylar flare of the distal femur. We prefer this exposure to a percutaneous technique. It allows direct visualization of the entry site, which makes the nail insertion easier and safer. It also allows the nail ends to be advanced sufficiently so that they are not prominent under the skin. It also minimizes the trauma to the overlying muscle, which could contribute to pain at the insertion site and delay the recovery of knee range of motion.
The entry site for the nails is 2.5 to 3 cm proximal to the distal growth plate. The entrance hole can be created with a 4.5mm drill or a narrow bone awl taking care not to slip posteriorly. Once the drill bit or awl has penetrated the cortex it must be angled obliquely in a proximal direction. The more vertically the starting hole is directed, the easier it is for the curved nail tip to be deflected off the far cortex and advanced proximally. The awl or drill bit is removed. The contoured nails mounted on t-handled or universal chuck are then introduced into the distal femur through the starting holes, which are easy to find due to the exposure. The nails are advanced into the distal femur through the starting holes, which are easy to find due to the exposure. The nails are advanced either manually or with the mallet until both nail tip is not penetrating the far cortex. The nail can be slightly withdrawn and the curved tip turned away from the cortex to allow it to be deflected upwards rather than through the cortex.
Fracture Reduction:The nails in the distal femur can be used as a very effective traction device to facilitate the reduction of the fracture. With the hip flexed and the thigh supported as described, the handle of the chuck holding each nail can be pulled back and up. There is sufficient friction between the nails and the femur that the nails will not back out while traction is being applied. The distal femoral segment can be pulled out to length, flexed or extended, angulated into varus or valgus or rotated using the chuck handles. Under image guidance, the medullary canal of the distal femur is brought into alignment with the medullary canal of the proximal femur. Even as the traction is being applied to maintain the alignment, the nails are advanced with the mallet until the nail tips are across the fracture site. When there is only partial overlap of the distal and proximal canals, the chuck handle can be turned so that the curved nail tip is appropriately directed towards the proximal medullary canal. Once the nail is advanced across the fracture site the nail is untwisted until the tip is pointed to the original direction by reversing the turn of the chuck handle.
The first nail across the fracture should not be advanced more than 2 or 3 cm beyond the fracture until the second nail has been advanced across well. If this is deferred it is likely to displace or angulate the fracture often making it very difficult to get the second nail across. The nail introduced from the lateral side is directed to the base of the greater trochanter, while the medical nail is directed medically into the femoral neck. Adequate intra-operative imaging of the entire femur including the hip, in both antero-posterior and lateral projections is imperative to confirm the intramedullary location of the nails and to ensure that the tips of the nails have not perforated the cortex of the femoral neck.
Nail Trimming:Once the nails are fully inserted the distal nail ends should not be bent outwards. We have shown that the practice of leaving nail tips prominent to facilitate subsequent removal of the nails, as illustrated by the originators of this technique, inevitably produces symptoms at the insertion site. These symptoms will necessitate removal of the nails, sometimes prior to fracture union. The objective is to trim the nail so that its end is not prominent under the skin, and yet out far enough from the bone entrance hole to facilitate subsequent removal should this be necessary.
In the fully inserted position the desired position of the cut is marked on the nail. The nail is than withdrawn sufficiently to cut it at this level. The nail is then re-advanced with a hollow punch so that its end lies adjacent to the supracondylar flare of the distal femoral metaphysis. The knee is put though a full range of motion to ensure the ends of the nail do not bind on the overlying muscle or iliotibial band. Once the incisions are closed the end of the nails should not be palpable under the skin. It is important to note that the nail ends are not buried within the bone but remain outside the actual cortical entry site between 1.0 to 1.5 cm. Elective removal can still be accomplished quite readily with currently available extraction devices. If the nail entry site is too low the end of the nail will lie beside the epicondyle and therefore will become prominent and potentially irritable to the growth plate. Whether it is necessary to routinely remove flexible nails implanted in children is unclear. Our current practice is to remove only those nails associated with symptoms.
Postoperative Management:Patient is encouraged to perform active knee range of motion and static/isometric quadriceps exercises. Weight bearing on the injured limb is limited to the weight of the leg with the foot just resting on the ground (“toe-touch” or “touch down”). The child can be discharged when he/she is able to ambulate, which is between 3 to 5 days. Radiographs are obtained 2 weeks after fixation and again at 6 weeks. There is usually bridging callus noted at this time and the patient is allowed to gradually increase to full weight bearing as tolerated over the subsequent 4 weeks. Radiographs are repeated between 10 to 12 weeks after surgery, when most fractures have healed. Crutches are no longer required and patient can begin to return recreational non-contact sports as tolerated.
Fractures with fragmentation > 25%, proximal (sub-trochanteric) fractures, or long spiral fractures can be treated by this technique but should be monitored carefully to detect early loss of reduction and to prevent possible malunion. These fractures might benefit from additional external immobilization. We use removable knee immobilizers for the first 6 weeks or until callus formation. By limiting the motion at the knee, hip motion is all reduced significantly which indirectly protects the fracture by limiting the overall motion at the knee, hip motion is all reduced significantly which indirectly protects the fracture by limiting the overall motion of the femur. Patient can remove the immobilizer to shower and to work on gentle active range of knee motion after 2 weeks. The patients are followed more frequently at 1, 2 weeks and 4 weeks after their operation, with radiographs to rule of any change in alignment.
References:- Sanders JO, Browne RH, Mooney JF, et al. Treatment of femoral fractures in children by Pediatric Orthopedists: Results of a 1998 survey. J Pediatr Orthop 2001; 21:436-441.
- Wright JG. The treatment of femoral shaft fractures in children. A systematic overview and critical appraisal of the literature. Can J Surg / J Chir Can 2000; 43:180-189.
- Ligier JN, Metaizeau JP, Prevot J. Closed flexible medullary nailing in Pediatric traumatology. Chir Pediatr 1983; 24(6): 383-5.
- Metaizeau JP. L’osteosynthese chez l’enfant par embrochage centro medullaire elastique stable. Sauramps Medical, Montpellier 1988.
- Ligier JN, Metaizeau JP, Prevot J, Lascombes P., Elastic stable intramedullary nailing of femoral shaft fractures in children. J Bone Joint Surg [Br] 1988; 70-B: 74-7.
- Bar-On E, Sagiv S, Porat S. External fixation or flexible intramedullary nailing for femoral shaft fractures in children. J Bone Joint Surg [Br] 1997; 79-B: 74-7.
- Flynn JM, Hresko T, Reynolds RAK, Blasier RD, et al. Titanium Elastic nails for Padiatric Femur fractures: A multicenter study of early results with analysis of complications. J Pediatr Orthop 2001; 21:4-8.
- Carey TP, Galpin RD. Flexible intramedullary nail fixation of pediatric femoral fractures. Clin Orthop 1996; 332:110-118.
- Heinrich SD, Drvaric DM, Darr K, MasEwen GD. The operative stabilization of pediatric diaphyseal femur fractures with flexible intramedullary nails: A prospective analysis. J. Pediatr Orthop 1994;14:501-507
9. Femoral Torsion
Prof. S.S. Gill,
Department of Ortho Unit II,
PGIMER,
Chandigarh.
The normal torsion or anteversion of the femur, its measurement and the clinical significance of it in various clinical conditions has been a subject of debate for a long time now. Some of these aspects are being discussed here briefly.
Normal Anatomy Of Proximal Femur With Regards To Torsion.Normally the femoral head and neck are not in the same plane as the femoral shaft and the condyles. The femoral neck is rotated anteriorly in the coronal plane to produce what is called the anteversion angle. The limb bud of the lower extremity appears during third week of embryonic life. The great toe is initially preaxial i.e. on the lateral side of the limb. Subsequently it medially rotates bringing the great toe to the medial side of the leg.The degree of anteversion is the greatest during infancy. It gradually decreases during postnatal life due to external rotation of the extremity.
Definition of Anteversion (av):The geometry of the femur and the definition of anteversion were described by Billing in the year 1954. It is necessary to know certain definitions to understand the angle of anteversion. The long axis of the axis of the femur is the line defined by two points: the centre of the knee (centroid through the distal femoral metaphysis in a cross section through condyles) and the centre of the base of the femoral neck. (the centroid of the femoral diaphysis in a cross section through the base of the femoral neck).The axis of the femoral neck is the line defined by two points: the centre of the femoral head and the centre of the base of femoral back. The plane of anteversion is the plane that contains both the long axis of the femur head and the centre of the base of femoral neck. The plane of anteversion is the plane that contains both the long axis of the femur and the axis of the femoral neck. The condylar axis is the line that is parallel to the posterior aspects of the femoral condyles and passes through the centre of the knee. The condylar plane contains both the long axis of the femur and the condylar axis. The angle of anteversion is the angle in the transverse plane between the plane of anteversion and the condylar plane.
Normal values of anteversion angle:
The mean value amounts to 11 deg with a range of 40-50 deg and a std deviation of 10 deg.
The mean value for the male femora is 2 ½ deg smaller than for the female femora.
The mean value for the left femora is 2 deg higher than for the right.
The differences between pairs of femora range from 0-15 deg with mean of 5 deg and std deviation of 3.5 deg. Approximately 10% show differences of 10 deg or more.
After closure of the growth plates, there are no further changes of the anteversion angle.
During the postnatal period the mean value is reduced from 30-40 deg to 10-12 deg. In this period the differences between pairs of femora belonging to the same individual are similar to the differences in adults.
Methods for measuring femoral anteversion:Measurement of anteversion angle is important for the diagnosis and selection of patients for derotational osteotomy.
Clinical methods:Netter in 1940 was probably the first person to describe a technique to measure anteversion angle clinically. A more recent method of measuring the same has been described by Ruwe et al in 1992. This is called trochanteric prominence angle test.
Technique:Pt is made to lie prone with the hip extended and the knee flexed to 90 deg. The hip is rotated internally while the examiner palpates the greater trochanter till its maximum prominence is palpated. In this position the neck of femur is parallel to the floor. The angle subtended by the tibia and true vertical representing the femoral anteversion is measured with a goniometer.
Radilogical methods:There are three methods to measure av angle by plain radiography. Flouroscopic Biplane radiography Axial roentgenography.
Flouroscopic method:Pt lies prone on fluoroscopic table with the hip extended and the knee flexed to 90 deg. The hip is externally rotated till the femoral head is directly in line with the femoral shaft. A gonimeter is used to determine the angle of torsion formed by the angle between the limb and the plane of the table.
Biplane method:(Dunlop 1953): Pt is placed on a special apparatus so that the hip is in 10 deg abduction and 90 deg flexion with 90 deg flexion at the knee. With this a lateral radiograph is taken. A PA radiograph is taken with pt in the prone position. With these x-rays, apparent angles of inclination and anteversion are obtained. The true angle of torsion is calculated by using these apparent angles by means of a trigonometric formula. Other biplane methods include Norman method, Rippstein’s method, etc.
Axial roentgenographic method:(Dunn 1952): Pt Lying supine position the hip and knee are flexed to 90 deg. The x-ray beams are directed vertically so that the femoral condyles seem superimposed on the femoral neck. The angle between the transcondylar plane and the neck is measured directly on radiographs.
Drawbacks of plane radiography:Errors can occur due to asymmetric position of the patient and inexact abduction. Possible rotation of the femoral condyles during position changes. In axial radiography excessive irradiation required to produce adequate x-ray.
Ct scan:This is presently the gold standard for the measurement of av angle. Recent methods described by Murphy et al uses the following sections in the femur.
A scout view is taken from which the femoral length can be determined. Axial cut through the largest diameter of the femoral head, marking the centre of the best-fit sphere. Several millimeters proximal to the lesser trochanter, marking the centroid defined as the intersection of centrally placed lines in the anteroposterior and the mediolateral planes. At the level of the distal femoral condyles where a line is constructed joining the most posterior point of each condyle. Using CT software cuts 2 and 3 are superimposed and a new line is constructed. The angle subtended by line 2-3 and line 4 corresponds to femoral anteversion. The measurements by CT scans have been found to be very accurate.
UltrasoundTechnique:
Pt is made to lie supine with the knee flexed to 90 deg over the edge of the table. The transducer is place on the anterior aspect of the centre of the femoral head and GT. The transducer is tilted in the plane of the ultrasound beam until the tangent of the femoral head and the GT appeared horizontal on the screen. The degree of tilt of the transducer is measured using a clinometer. The measured av angle is equal to the angle of the tilt. Ultrasound consistently overestimates the av angle and so correction factors have been introduced: subtract 4 deg in children and 10 deg in adolescents and adults from the measured av angle.
Advantages:Rapid, safe, painless, no radiation exposure, a single scan is enough to measure the angle.
Disadvantage:Not very accurate. Ultrasound methods have therefore been recommended as a screening technique for patients with rotational deformities of the femur.
MRI:Recent studies indicate that MRI has the same accuracy precision and reliability as CT scan.
Advantages:Superior in evaluation of infants in whom the head and neck are cartilaginous. No radiation.
Disadvantages:More time consuming (30 min). May need sedation in children. Costly MRI could replace CT scan as the gold standard.
Clinical significance of femoral torsion.:Fractures of the femur and the tibia: In association with the fractures of the femur, torsional malunion have been found to be present in upto 30% of the cases in many of the follow up studies. Recent clinical and experimental studies have shown that remodeling of the rotational malunion does occur.
Medial femoral torsion: The measurement of torsion is important to decide on the need for derotational osteotomy and how much of it should be done. Staheli has listed the following indications: Persistent severe disability in a child greater then 8 years. Deformity severe enough to create significant functional and cosmetic deformity. Measured av angle more than 50 deg. Medial hip rotation greater than 85 deg and lateral rotation less than 10 deg.
Torsional malalignment syndrome: It is a combination of increased femoral anteversion and increased tibial lateral torsion. This condition may lead to patellofemoral mal-alignment and chondromalacia. Conservative treatment has been advised in most of the cases.
DDH: It has been found in studies that children with DDH have an increased anteversion angle on the affected as well as the normal sides. On long term follow up studies it has been inferred that if a markedly increased anteversion is discovered in a child with a dislocated hip, a spontaneous correction to normal cannot be expected. But none of them show high values that warrants surgery.
Coxa vara: In a study by Shands and Marshall,m it was found that coax vara was associated with marked decrease in femoral torsion. In a few cases even retroversion was found.
Cerebral palsy: In these children the av angle usually measured more than normal value and on follow up no significant decrease of torsional deformity was found. The increased av angle is believed to be due to abnormal muscle tone. Also it has been studied that the excessive anteversion is usually responsible for the apparent coax valga in AP radiographs of pts with CP.
Coxa valga: In many follow up studies it has been found to be associated with increased femoral torsion.
Perthes Disease: In most of the studies, it has been found that only about 15-20% of the cases showed an anteversion of 10 deg above normal in the affected side. But some studies (Craig et al 1963) showed an increased average av angle of 45 deg and postulated that the disease was due to pressure necrosis on the anteverted head. This was not supported in later studies.
Idiopathic osteoarthritis of the hip: Though it had been hypothesized that medial femoral torsion is a predisposing factor for this condition, it was clear from various studies that the association was not statistically significant and that rotational osteotomies should not be performed in children as a prophylactic measure except when indicated.
Conclusion:Orthopaedist and anatomist have long been interested in the angle of anteversion of the femoral neck. Excessive femoral anteversion is a common developmental deformity affecting rotational alignment of the lower extremity in children on an idiopathic basis or due to muscle imbalance in certain neuromuscular disorders. The best method to measure femoral torsion was controversial. This has cleared certain extent. Of the available methods today computerized axial tomography satisfies the criteria of accuracy and technical suitability. It is currently considered the gold standard for this purpose but could be replaced by MR imaging in the future because the latter enables more accurate, precise and reliable measurements especially in infants in whom the head and neck are cartilaginous. The degree of femoral anteversion has been thought to be very important in CDH, cerebral palsy, Perthes disease and other neuromuscular disorders. Its measurement became important when femoral osteotomy started being advocated to correct the excessive medial torsion on these disorders. There has been many studies trying to figure out the importance of increased anteversion in these disorders. However still many controversies exist in its management and is subject of ongoing research.
10. Genu Varum & Valgum and Angular Deformities of Leg
Prof. A. Devadoss
Institute of Orthopaedic Research and Accident Surgery
MADURAI
The topic of discussion in this paper represents the very essence of orthopaedics as contemplated by the person who coined the word “orthopaedics”. In 1771, an 83 years old Parisian pediatrician Nicholas Andry wrote a self help book for parents with the title “Orthopaedia, or the art of correcting & preventing deformities in children: By such means as may easily be put in practice by parents themselves, & al such as are employed in educating children”. The symbol of orthopaedics is Andry’s tree – he was trying to keep the legs of rickety children straight hence the analogy to a young tree.
In 1855, Edward Lonsdale reported on the diagnosis of 3000 patients that he & Dr. Adams treated at the Royal Orthopaedic hospital in London.
Bow legs & Knock knees – 1663
Club Feet – 495
Deformities of Spine – 465 etc.
Dietary rickets was common during this time & that was the cause of Genu varum & valgum at that time. The bow legs & knock knees we see today are entirely different from what was seen and reported by Lonsdale.
Deformities of the tibia & fibula are the most obvious and most commonly brought for orthopaedic opinion because of the real or apparent detrimental effect it can have other the child’s joint. Most deformities are physiologic and the real job of the orthopaedician is in differentiating the pathologic from the physiologic forms of Genu varum/ valgum.
GENU VARUM:Deformities at the knee can be due to deformities at the distal femur or the proximal tibia. The importance of differentiation is obvious as the treatment adopted will depend on the location of the deformity. This can be simply done by examining the knee in extension and in flexion. Femoral deformities will be masked by flexion as the tibia rolls back to articulate with the posterior aspects of the femoral condyles. This paper will discuss tibia vara ie. Deformities at the knee due to proximal tibial problems.
Thomson et al has described 4 types of tibia vara
- Infantile (Blount’s disease)
- Juvenile (4-10 yrs)
- Adolescent (> 11 yrs)
- Focal Fibrocartilagenous Dysplasia
The normal tibio-femoral angle develops in a child as the child grows. Selenius (1972) in a classic study has described the development of the varus (180) in a child between 0-18 months into a valgus of about 18 between 2 years to 6 years which then settles into a normal physiologic knee alignment of 70 of valgus by 7 years of age.
A young child with a normal varus walks with a broad based gait in the first few months of walking (10-18 months) the forces on the medial tibial physis far exceeds the forces on the lateral and according to the Hueter-Volkmann principles the varus tends to get exaggerated. As the broad based gait narrows the varus because valgus and then settles to the physiologic level.
Blounts disease will be dealt with extensively by others. The juvenile form of the tibia vara usually develops due to physeal plate injury due to trauma or infection. There is continued over growth of the lateral aspect of the physis as compared to the medial producing a deformity. There is a lot of controversy as to whether the juvenile diopathic form is an infantible tibia vara (Blounts disease) which was recognized late. But onset of the deformity after 8 years will definitively constitute adolescent tibia vara. The response to osteotomy of the adolescent form is much more favourable than the infantite or the juvenile forms.
Trauma & infections are not considered factors producing adolescent tibia vara, unless obesity causing increased pressure on the medial epiphysis in considered chronic trauma!
Histopathologically biopsy specimen of medial physis show evidence of fissuring and clefts in the physis, fibrovascular & cartilaginous repair tissue at physeal – metaphyseal junction & sequestered islands of hypertrophic chondrocytes. These finding are consistent with microscopic damage secondary to mechanical compression according to the Hueter-Volkmann principle. True bony bridges have rarely been demonstrated.
Clinical features:An obese teenager whose weight exceeds the second standard deviation above the mean are greatly predisposed. There is a male preponderance. The reason is unknown. It may be unilateral or bilateral and patients are essentially asymptomatic. Internal tibial torsion of varying degree is usually frequently present. Limb length discrepancy is usually present and the choice of treatment may be influenced by discrepancy greater than 2.5 centimetres.
Radiology:The shape of the tibial physis is relatively normal. The sine qua non is the widening of the proximal medial physeal plate. In addition there may be widening of the lateral distal femoral physis. This traction widening of the lateral side of the varus deformity would appear consistent with Delpech’s raw although interestingly there is no widening of the lateral proximal tibial physis. Lack of sloping or inferior braking of the medial proximal tibia differentiates it from infantile tibia vara.
Treatment:Is predominantly surgical weight loss is desirable and should be recommended.
Tibia vara secondary to focal firbocartilagenous dysplasia:Occasionally in infant or toddler may present with a unilateral tibia vara with deformity slightly more distal at the joint itself. Hypertension of the knee may also be present which differentiates it from infantile tibia vara.
Radiology:A characteristic abrupt varus at the metaphyseal diaphyseal junction is seen clearly not involving the physis. There is cortical sclerosis at this area with a radiolucency just above this are at the insertion of the pes anserine tendons which corresponds to the firbocartilage tissue found at surgery.
Treatment:The importance of recognizing this condition from tibia vara is that the deformity often revolves spontaneously, surgical treatment is necessary if the deformity progresses or fails to resolve during period of observation with orthotic management.
Genu Valgum:A valgus alignment at the knee is normal in a child between 2 –7 years. After 7 years correction of excessive physiologic genu valgum may be indicated when there is gait disturbance, difficulty in running, knee discomfort, patellar mal-alignment, evidence of ligamentous instability or excessive cosmetic concern.
 Treatment options:
Treatment options:
Include hemiepiphyseodesis (Temporary with staples or transphyseal screws, or permanent using time epiphyseodesis) has the advantage of producing unilateral physeal inhibition achieving correction gradually and close to the joint where correction will be most effective. Several different forms of hemiephiphyseodesis has been described. However possibility of overcorrection due to overgrowth is always present. The use of Green Anderson growth charts and Bowen angular correction tables have been described. Our experience with this procedure is limited. We do not follow this any more. A corrective osteotomy at the distal femur is the treatment of choice.
Genu valgum secondary to proximal tibial fracture:Post traumatic tibia valga was first reported in 1953 by Cozen. Several explanations for this phenomenon has proposed including soft tissue interposition at the fracture site, growth stimulation at the medial physis and tethering of the lateral physis by the intact fibula or Ilio-tibial band.
Treatment:Open reduction – in order to extract interposed soft tissue has not been successful in preventing the subsequent valgus. Ideal treatment is by immobilization in a varus molded long leg cast. Patient should be kept under observation for several years. The maximum deformity is reached at about usually 1 year and spontaneous improvement occurs over several years. Surgical treatment should be delayed as much as possible. Hemiepiphyseodesis or osteotomy may be contemplated. Physeal injuries leading to tibia valga may be treated by bony excision and fat/ silastic interposition or by chondrocyte transfer at the physeal plate.
Bowing of the Tibia:Bowing of the diaphysis of the tibia is usually noted at the birth and the term congenital is appropriate. Three types are recognized.
1. Antero-lateral bowing – without pseudoarthrosis (Benign) or with limb threatening condition like pseudarthrosis
2. Postromedial bowing
3. Anterior / antero-medial bowing with congenital deficiency of fibula.
Antro-lateral bowing of the tibia with pseudoarthrosis will not be considered here. The benign form is usually progressive and casting may be tried in the early stages. When the patient is seen later multiple osteotomy with intramedullary fixation is the treatment of choice. Invariably there is some medullary sclerosis & intramedullary fixation may be difficult. The fixation usually includes immobilization of the ankle for stability of the small distal fragment.
Late fracture:Occasionally a child present with a tibial fracture that fails to heal following cast immobilization. Usually there is no prior history of the abnormality of the tibia, however radiographically it may be dysplastic. Sometimes the presenting symptom is pain in a stress fracture seen radiologically. The outcome following treatment of such late fracture in previously undiagnosed dysplastic tibia is generally more favourable than the outcome of treatment of conginetal pseudoarthritis. Treatment with external fixation devices or vascularised bone tissue transfer are the options of choice. The benign form of antrolateral bowing my spontaneously resolve is 1% of children, a pattern which is more common with conginetal posteromedial bowing. In this group radiographs demonstrate a presumptive healing response in the concavity of the bone consisting of hypertrophy and subperiosteal new bone formation. Additional radiographic findings that identify this pattern includes fibula which is straight and long and uninvolved with the bowing and the foot maintained in a relative varus position unlike the valgus pattern seen with the true pseudoarthritis of the tibia. Discrepancies exceeding 5cm at maturity are not unusual and limb lengthening is the treatment of choice.
Congenital posteromedial bowing:This deformity is usually present right from birth and usually associated with a calcaneus foot. It is almost certainly due to intrauterine malposition. The calf is frequently smaller in diameter with a dimple at the apex of the angulation. A posteromedial bow is usually a single deformity without associated conditions or anomalies. The natural history of the bowing is spontaneous resolution especially during the 1st six months – 2 years the posterior bowing should be completely resolved though the medial bowing may take a few more years. For deformity usually resolves by 9 months. Shortening commonly exceeds to 2.5cms
Treatment:Initial treatment includes a gentle stretching of the dorsiflexion contracture as well as lateral ankle structure into a supinated and inverted position. Serial casting may be used more for the satisfaction of the parents then as the method of treatment. Stimulation exercises of the plantar flexors may be helpful. Orthotic devices are usually helpful to correct the limb length discrepancy. No treatment should be considered until a adequate period of observation confirms that correction is infact not occurring. Severe residual deformity after an age of 3-4 years is an indication for corrective osteotomy. Limb lengthening is performed at a later date for limb length equalization.
11. Management of Genu Varum Diagnostic and Treatment aspects
V.V.J. Soma Raju, Benjamin Joseph
Paediatric Orthopedic Service, Department of Orthopaedics,
Kasturba Medical College, Manipal.
Bow legs are one of the commonest complaints in the toddlers. Fortunately most often they prove to be harmless and self-correcting with further growth and maturity of gait. But before reassuring the parents, we need to rule out the less frequent but more harmful conditions which need early diagnosis and management for optimal results.
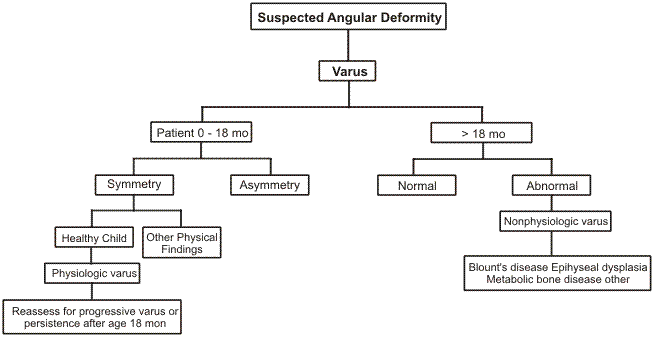
Natural history of tibio-femoral angle (TFA):Bowlegs and medial tibial torsion are normal in new born and infants. The TFA at birth is 10 to 15 degrees of varus and its remodels to neutral by 18 months of age. Genu valgum develops with further growth and the TFA reaches 12 degrees of valgus by the age of 3-4 years. The TFA swings back to the final adult values of 8 degrees in female and 7 degrees in male by the age of 7 ears. Interference in any phase of this swing may result in angular deformities of leg. The TFA has certain variability among normal individuals. To differentiate the normal extremes form the abnormal Sharrard proposed simple guidelines, “Persistence of bilateral genu varum (inter-condylar distance > 10 cms) beyond 3 years of age and genu valgum (Inter-malleolar distance > 10 cms) beyond 10 years and unilateral knock knee and a varus angle (with inter-condylar distance > 5 cms) are abnormal and needs further assessment”. But even earlier diagnosis became desirable in Infantile Tibia Vara. Early diagnosis allows the consideration of arresting the progress with brace treatment, and early corrective surgery when indicated is critical in achieving restoration of normal growth.
Evaluation of persistent genu varum:History:
A positive family history may indicate congenital familial tibia vara, while the short stature of the parents may suggest the possibility of dysplasia or growth disorder. The age at which the deformities are first noticed, and their course since then will provide the ground information. History of early walking is common in both infantile tibia vara and physiological genu varum.
Examination:Short stature suggests Rickets or bone dysplasia. Alignment of the limbs is assessed in standing and then in supine position. Disappearance of bowing when knees and hips are extended fully and rotated to neutral position with patellae facing forward suggests apparent genu varum. Improvement of alignment in supine position indicates lateral ligamentous laxity. The inter-condylar distance should be recorded with knees straight and ankles just touching each other. Lateral thigh angle may be measured with a long gonimeter.
Site of varus angulation:
A gentle curve with more pronounced bowing in the lower third of the femur and at juncture of middle third and lower third tibial shaft suggests – Physiological genu varum.
At the Knee joint – Ligamentous laxity
Acute medial angulation immediately below the knee – Tibia vara
Lower tibia at the junction of middle third and lower third – Congenital familial tibia vara
Distal femoral epiphysis – Rare distal femoral vara
Physiological genu varum and congenital tibia vara deformities are usually bilateral ad symmetrical. In Blount’s disease even when both legs are involved the degree of bowing is often asymmetric.
Limb length discrepancy:Limb lengths are even in Physiological genu varum whereas in infantile tibia vara the involved or the more affected leg is shorter.
Gait:Lateral thrust in stance phase with upper tibia shifting laterally indicates laxity in incompetence of lateral collateral ligament. Lateral thrust develops with progression of infantile tibia vara.
Radiographic evaluation:Indications for an x-ray:
- The varus deformity is not improving or is getting worse in a three old.
- The bowing is unilateral or asymmetric.
- The varus angulation is acute, immediately below the knee
- Positive ‘Cover up’ test
- In presence of clinical features suggesting pathologic genu varum
- Short stature, Enlarged physis, history of trauma/infection & Presence of lateral thrust.
The radiograph should be a Standing long film that includes hips, knees and ankles with knees straight and patellae facing forward. To get this position the feet may need to be turned in to neutralize the effect of internal tibial torsion on the radiological measurements.
Differential diagnosis of bow legs:
Apparent genu varum - Rickets
Physiological genu varum - Bone dysplasia
Congenital familial tibia vara - Fibrocartilagenous dysplasia
Tibia vara (Blount’s disease) - Asymmetric growth arrest
In addition we had a group of children in whom the varus deformity progressed in absence of classic radiological features of Blount’s disease to the extent that needed surgical correction of the deformity. Many of them had lateral ligamentous laxity. Ronald John Kendig has noted that “Unexplained large angular deformities are common in developing countries without apparent current metabolic abnormality or excessive body weight. He postulated that transitory nutritional factors might play a role in triggering the deformity which is then accelerated by mechanical factors”. In absence further knowledge we termed this group of patients as “Exaggerated Physiological genu varum”.
The clinical and radiological features an readily differentiate metabolic bone disease and bone dysplasias from physiological genu varum. Clinically we use the ‘cover-up’ test (Davids et al, JPO-2000) for screening the bowleg deformities. But the radiographic changes of Infantile tibia vara before the classic radiological changes appeared. Levine and Drennan introduced Tibial Metaphyseal-Diaphyseal Angle (TMDA) and found it useful with a false positive rate of 3%. But later studies by Feldman and Schoenecker, James J McCarthy et al found the false positive rates to be unacceptable high (>30%) when the TMDA > 11 degrees is taken as diagnostic for Blount’s disease. Feldman and Schoenecker showed that by restricting the use of TMDA only when it is (<)9 degrees to suggest Physiological genus varum, and >16 degrees to indicate Infantile tibia vara, the false positive and negative error can be reduced to (<)5%. But a large percentage of the patients in their series fell into this gray zone (33-42%). In our cases, the over malalignment (TFA) was comparable in both Physiological genu varum and Tibia vara. But, most of the deformity (74%) was present at the proximal tibial metaphysis in children with Blount’s disease, but quite significant (35%) in children with Physiological genu varum. We concluded that the metaphysio-diaphyseal angle at the distal femur (MDA-DF) helps in differentiating these tow conditions at an early stage (POSI-1999). Later at the distal femur (MDA-DF) helps in differentiating these two conditions at an early stage (POSI-1999). Later James J McCarthy et al (JPO, 2001) used the ratio between metaphysio-diaphyseal angles at distal femur and proximal tibia and described the femoral tibial ratio (FTR) which compares the amount of bowing that occurred at the distal femoral metaphysis to that present at the proximal tibial metaphysis. In their series FTR has less false positive and false negative rates compared to the Tibial metaphysio-diaphyseal angle (TMDA). Another limitation of the TMDA was that it can be significantly affected by rotation (Henderson et al). By using FTR the effect of rotation was reduced. FTR managed to diminish but not erase the gray zone.
Management:Management depends on the diagnosis, age of the patients, stage of the disease, remaining growth potential, degree of varus deformity and joint laxity. Metabolic bone disease needs accurate diagnosis and correction of the metabolic disorder. Residual bow deformity should be managed conservatively if it is not severe and remaining growth potential is significant. Operative correction should be considered in persistent or progressive deformity once the underlying disorder is corrected. Fibro cartilaginous dysplasia is usually self correcting with further growth and orthotic support is usually sufficient.
Persistent bow legs in the child between two and three years should have radiographs especially in presence of other risk factors. If the child is in the Gray Zone (TMDA between 9-16 degrees and FTR between 0.7 and 1.4) presence of other risk factors influence the decision. Simple observation with periodic follow up is advised when
- TMDA < 11 degrees
- FTA > 1.4
- Absence of irregular radiolucencies in proximal tibial epiphysis
- No lateral thrust
- Medial tibial torsion of < 30 degrees
- TMDA > 15 degrees
- FTR < 0.7
- Presence of lateral thrust
- Presence of irregular radiolucencies in proximal tibial epiphysis
- Unilateral, progressive deformity
- Internal tibial torsion > 45 degrees
Brace treatment may not be suitable in very obsess and especially when bilateral. Over the age of 3 to 4 years brace treatment is not advised as it may not be possible to get the correction before the age of 4 years which is critical in restoring growth patterns.
Valgization osteotomy:- Age above 4 years
- Advance Blount’s disease (Langenskiold stage = or >III)
- Non-compliance with brace treatment
We routinely used Rib’s technique of oblique tibial diaphyseal osteotomy. It allows correction of angular as well as rotation deformities. In younger children no internal fixation was used. Minimal internal fixation was used in older children. Elevation osteotomy of medial tibial plateau was done in one case with advanced Infantile tibia vara with physeal sloping. We noticed under correction in initial case with infantile tibia vara. Intra-operative radiograph may be useful in preventing this. Epiphysiodesis may be useful in the management in adolescent tibia vara. External fixator application is needed in adolescent tibia vara for deformity correction and limb. Lengthening
Bibligraphy:- Jon R Davids, Dawn W Blackhurst, Benjamin L Allem Jr. Clinical Evaluation of Bowed legs in Children. J Pediar Orthop 2000; 9:278-284.
- Alan M Levine, James C Drennan. Physiological bowing and tibia vara. J Bone joint surg Am 1982; 64-A:1158-1163.
- Michael D Feldman, Perry L Schoenecker. Use of Metaphyseal-Diaphyseal Angle in the Evaluation of Bowed legs. J Bone joint surg Am 1993;75-A1602-1609.
- Henderson RC, Lechner CT, DeMasi RA, Greene WB. Variability in radiographic measurement of bowleg deformity in children. J Pediatr Orthop 1990:10:491494.
- James J McCarthy, Randal R Betz, Andrew Kim, Jon R Davids, Richard S Davidson. J Pediatr Orthop 2001; 21:545-548.
- Rab GT. Oblique tibial osteotomy for Blount’s disease (tibia vara). J Pediatr Orthop. 1988; 8:715-720.
12. Classification of Congenital Limb Deficiencies
Dr. Bhasker Banerji
Consultant Orthopaedic Surgeon, Allahabad.
The Thalidomide Disaster brought into sharp focus the multitude of congenital limb deficiencies, which may occur. It also brought into focus the lacunae that existed in the world of medicine – in terms of toxicity of drugs used during pregnancy and the limitations that existed regarding the management of such conditions. More important was even the lack of terms that were used to describe these deformities.
Frantz and O’Rahilly (1961) made the first effort at classification of congenital limb deficiency. His nomenclature contained many Greek and Latin words which created a confusion of interpretation, when used in European languages, other than English. The word “hemimelia” in particular causes confusion. It literally means “half a limb”. This may be interpreted as “present” or “absent” or “affected” in different language translations. In 1966 an effort was made to revise the classification by substituting the word “meromelia” instead of “hemimelia, to describe partial limb absence. This too developed certain terminology problems.
Swanson (1964) proposed a third classification. This too added further confusion particularly German translations. In order to do away with these confusions and to develop a simple easily communicable, documentable and translatable that the Current classification of the International Standards Organization was evolved.
The current classification:The current classification of limb deficiencies at birth is known as “International Standards Organization (ISO) Terminology”. This is a major change in the terminology used conventionally.
Need:The varying terminology used in different parts of the world, and the different and sometimes confusing words used by related professions in the world of medicine, made it necessary to develop a simple terminology. This would ensure uniformity in translation of the terms to languages other than English.
It was found that while describing similar clinical situations the previously accepted terms for amputation levels and congenital deficiencies were derived from different origins and unrelated terminology. For e.g. description of an amputation / deficiency at middle Tibia would be ‘below-knee amputation’ for an acquired amputation but would be called ‘terminal transverse partial hemimelia’ for lower-limb-amputation for a congenital limb deficiency. Not only are both confusing but they are also difficult to translate to other languages. This is why the current terminology was developed, and it is a major change from the terms conventionally used.
The Terminology per se”:The International Standards Organization is an international body that lays down uniform standards for items, processes, terminology etc. which can be easily duplicated and understood. Numbers are used to indicate which ISO Standard is being discussed.
The standards, which were used to reach this classification, were ISO 8548 and 8549, and relevant subsections of them.
The terms above knee, below knee etc., used to describe amputation have been now been replaced by the new terminology. This uses three adjectives; trans, disarticulation and partial.
The adjective, “trans” is used when the amputation is across the axis of a long bone e.g. trans-femoral or trans-humeral. In the two cases where there are two contiguous bones, tibia/fibula and radius / ulna, only the primary or large bone is identified (e.g., trans-tibial, trans-radial).
The adjective “disarticulation”, is used when anatomically, the amputation is through the center of a joint (e.g. knee disarticulation, ankle disarticulation).
The use of proper nouns has been discontinued in the ISO terminology e.g. Symes amputation. This would now be referred to as ankle disarticulation. Any amputation distal to it would be partial foot amputation.
For upper limb acquired amputation levels as per the new terminology reads (from proximal to distal). Forequarter, Shoulder disarticulation, Trans-humeral, Elbow disarticulation, Trans-radial, Transverse carpal, Partial hand etc. For Lower extremity it reads: Hemi-pelvectomy, Trans-femoral, Knee disarticulation, Trans-tibial, Ankle disarticulation, partial foot etc.
ISOO 8548 –1 Method of describing Limb Deficiencies present at birth. In this terminology, all congenital limb deficiencies fall into one of the two groups: Transverse Longitudinal. The Transverse deficiencies resemble amputation-type conditions that are characterized by normal development until the point of deficiency beyond which the normal anatomy does not exist. In the case of the long bones of the arm, thigh, forearm and e-the transverse deficiency is described by naming the long bone and general location with regard to the long bone, such as complete (total), upper, middle or lower third (e.g. transverse deficiency of the left thigh lower third would be the term applied to long above knee amputation that terminates the distal third of the femur).
For transverse deficiencies that terminate in the carpal, tarsal, metatarsal and phalangeal are only designations, complete and partial are used (e.g. if one row of carpals remained, the terminology would be transverse deficiency-carpals-partial)
The longitudinal limb deficiencies are characterized by absent skeletal anatomy within the long axis of limb and in some cases include normal anatomy distal to the affected bone. The longitudinal deficiencies named by the bones affected in a proximo-distal sequence, and terms indicate whether each bone is totally partially absent, for metacarpal and metatarsal bones and their respective phalanges, the number of the digit affected is stated by the number (by numbering the digits from the radial or tibial side respectively and numbering of thumb or great toe as “1”). So partial absence of the right fibula would read as longitudinal deficiency of the right fibula-partial. Similarly absence of the radial side of the right forearm and absence of two rays would read “longitudinal deficiency of right radius, complete; carpals partial; metacarpals 1,2 complete; phalanges 1,2 complete.
13. Congenital Femoral Deficiency
Dr. Ashok Vaishnavi
Congenital Femoral anomalies usually involve the proximal femur and it is a spectrum of severity of femoral deficiency and deformity. It includes Proximal focal femoral defiency (PFFD), developmental coxa vara and congenital short femur.
Proximal Femoral Focal Deficiency:PFFD is characterized by shortening of the femur and a defect in the proximal femur, which is either unossified cartilage or a true discontinuity. Existing classifications are descriptive (Aitken’s, Gillespie, …….) but are not helpful in determining treatment protocols like reconstruction. These classifications are inaccurate in predicting the final femoral morphology based on the initial radiograph. Also they are designed with prosthetic replacement surgery in mind. Dror Paley’s classification is based on factors that influence lengthening reconstruction of the lesion. Knee joint mobility / deficiency, rather than hip joint mobility / deficiency is the most important factor determining functional outcome and reconstructability of CFD. The etiology of this condition is unknown, it may be a multifocal teratogenic process. The only known teratogen is Thalidomide. On physical examination the affected proximal femur of the limb is flexed, abducted and externally rotated. 15% have bilateral involvement and over 50% have anamolies distal to femur especially paraxial fibular hemimelia, absence of lateral rays of the foot and tarsal coalition.
Evaluation of the Infant With CFD:The Hip: Determine the presence of head or a Psuedoarthrosis either mobile or stiff. The presence of a well developed acetabulum is the best clue that the femoral head is present and mobile, M.R.I., and sonography are helpful, however Arthrogram is still preferred by many.
The Knee: Range of motion is a critical feature. Mobile knees should also be evaluated for stability of the tibiofemoral joint and tracking of the patella.
Treatment: Treatment must correct as many as possible of the four functional defects in PFFD:
- Major limb length inequality (if unilateral)
- Pelvic - femoral instability
- Malrotation of the lower extremity, including hip flexion – abduction - external rotation and knee flexion contracture
- Proximal hip muscle weakness.
In past in patients with unilateral PFFD, treatment was geared toward fitting a prosthesis. However with limb lengthening & reconstructive procedures gaining ground the aim is to find out the final length of the limb and based on it try to equalized the limb and also give a good useful limb. The strategy of management of all type cases is to convert 1b to type 1a and type 1a – 1 or worse into 1a-0. The strategy of management in type 2 cases is convert type 2a to 1a and in 2b to stabilize the hip by pelvic support osteotomy and then final lengthening. For type 3 – the goal of surgery is to convert a type 3a to type 2b and rest reconstruction as per type 2b. Prosthetic options may be preferable to minimize the complexity of treatment. One of the arguments for amputation and prosthetic fitting is the contention that limb reconstructive surgery leads to psychological scarring and loss of childhood. Limb reconstructive surgery is an investment. The child invests part of his or her childhood in order to live the majority of life as an adult with as near normal an extremity as possible. However successful limb reconstructive surgery requires a team dedicated to the type of treatment and should not be performed by a casual surgeon.
14. Tibia Hemimelia
*Sharaf Ibrahim, ** S Sengupta, ** Saw Aik,
+Abdul Razak, ++ James Hui, +++Toshio Fujii
**University Kebangsaan, Kuala Lumpur, Malaysia
+University Science, Kelantan, Malaysia.
++National University of Singapore, Singapore.
+++Fukuoka Children’s Hospital, Japan.
Congenital deficiency of the tibia (tibia hemimelia) is the rarest of the major congenital anomalies of the lower limb. It occurs in 1 in 1 million live births. It may be inherited and associated with medial duplication of the hands and feet. There is marked shortening and bowing of the leg, a flexion contracture of the knee and a rigid varus foot.
Jones et al (1978) classified tibia hemimelia into 4 types. 1n type 1a there is total absence of the tibia and the lower femoral epiphysis is markedly hypoplastic. With total absence there is a severe knee flexion contracture as the extensor mechanism is absent. Knee disarticulation is usually the only option.
In type 1b the distal end of the femur is well developed and the proximal tibia is present in cartilage, but not visible on early X-ray. The extensor mechanism is present and treatment can be similar to the type 2 patients.
In type 2 there is aplasia of the distal tibia. The proximal tibial anlage is present and knee extension is possible. Tibiofibular fusion is required for stability. The proximal fibula is centralized in the tibial cartilaginous anlage (Brown 1965) or a side-by-side tibiofibular synostosis can be performed. Because of the pronounced limb-length discrepancy and ankle abnormality, limb lengthening and ankle reconstruction are required.
In type 3 there is aplasia of the proximal tibia while in type 4, the tibia is short with marked diastasis of the distal tibio-fibula joint.
Compared to primary amputation, limb reconstruction for tibia hemimelia is a long and often arduous process requiring multiple operations and considerable periods of in-patient and out-patient care.
References:1. Jones D, Barnes J, Llyod-Roberts GC. Congenital aplasia and dysplasia of the tibia with intact fibula. J Bone Joint Surg 1978; 60B:31-9 Brown FW. Construction of a knee joint is congenital total absence of the tibia (paraxial hemimelia tibia) - a preliminary report. J Bone Joint Surg 1965; 47A:695-704
15. Fibular Hemimelia
Dr. G.S. Kulkarni
Fibular Hemimelia is a difficult problem and is classified by several authors. Paley’s classification, followed by us, is treatment oriented. Of the 17 cases, treated in this institution, 3 were adolescents and 14 were below 10 years of age. Soft tissue operation, radical postero-lateral release, was done in all children. Soft tissue release consists of 1) excision of fibular anlage, 2) contracted fibrous tissue 3) lengthening of tendo-achilles, peroneals 4) capsular release. 3 cases did not return for bony surgery, as the children started walking. In 8 children bony surgery, lengthening and correction of tibial bow, was done as a second stage. Amputation was done in 1 case, advised in 2 but refused. Paley suggests extensive surgery of soft tissue release, lengthening and correction of bow of tibia, supramalleor ostetomy and complete correction of foot deformity, including correction coalition of talus and calcaneum in 1 stage.
Treatment - Soft tissue only - 3 cases
Soft tissue release + bony - 8
Adolescent correction - 3
Amputation - 1
Refused - 2
Complete recurrence in 1 case, we had to do again both surgery of soft tissue and bone. Two surgeries were done in 3 and 3 in 4 cases. Complications are recurrence and pin tract infection.
Conclusions:Surgery is the treatment of choice. Radical soft tissue release, lengthening and correction tibia and foot deformity, Children tolerate the surgery well. Recurrece is common, requiring multiple surgeries.
Orthotic and Prosthetics in Congenital Limb Deficiencies
Balu Sankaran
Orthotics and prosthetics in skeletal limb deficiency:- The ISPO/ISO classification of congenital deficiencies for standardization of prosthesis of upper and lower extremities is presented.
- The most important aspects about children with limb deficiencies are discussed.
- The paediatric prosthetists selection for growth management strategies is discussed.
- In the lower limb prosthetists fittings for proximal femoral focal deficiency and the modifications of PFFD by a knee fusion and a Van Nees rotationplasty is illustrated.
- The fabrication of the footplate and provision of stability in the use of the prosthesis is discussed.
- Fibular hemimelias with a congenital pseudoarthrosis of the tibia fitted with a prosthesis is illustrated.
- An example of a fibular hemimelia with a congenital pseudoarthrosis of the tibia fitted with a prosthesis is illustrated.
- The features of the tibial hemimelia unilateral and bilateral is illustrated and a congenital Gritti Stokes amputation is demonstrated.
- Fitting of a Syme’s amputee and other levels of amputation in the foot is demonstrated.
- Upper limb deficiencies in children are presented (namely a radial clubbed hand and ulnar deficient upper extremity). A Myoelectric prosthesis and its use is demonstrated.
- The value of robotic aids is mentioned.
- The list of items available with Indian Manufacturers or with foreign manufactures manufacturing in India is displayed.
Free Papers - Abstracts
1. Radiological assessment of congenital talipes equinovarus (club foot) is it worthwhile?
Dr. Surendra U. Kamath
Associated Professor
Department of Orthopaedic Surgery
Kasturba Medical College Hospital
Attavar, Mangalore 575 001, India
E-mail – skamath3@hotmail.com
Controversy exists regarding the use of standard radiographs in the evaluation of congenital talipes equinovarus in infancy. This could be the result of complex triplane malalignments and impaired ossification of tarsal bones. To address this issue, a study was undertaken to look into the inter observer ad intra observer reliability of estimation of Talocalcaneal and Talometatarsal angles on standard radiographs done as per Simons method. The results of analysis showed significant differences between the measurements on two occasions by the same observer. Also there was a marked difference in the measurements between the two observers.
2. Modified chiari’s (parikh’s) ostoetomy in developmental displasia of hip or congenital dislocation of hip
Dr. Ashwin Parikh
Orthopaedic Surgeon fellow I.O.R (Italy) Paediatric Orthopaedics
Email-ashwinparikh@usa.net
Chairi’s osteotomy for congenital dislocation of the hip or developmental dysplasia of the hip is a very known technique.
At times one faces problems for inadequate acetabular roof formation by this technique or one may need more roof of acetabulum for entire head femur accommodation.
Parikh’s technique forms more roof laterally and superiorly so as to accommodate entire head femur in the acetabulum. Weight bearing is more adequate and better forming good anatomical and physiological support. This is a new and fully innovative technique.
No changes are made in lever-arm mechanism of hip. Thus glutei, neck femur and acetabulum are not much altered. Trendelenburg’s principal is not altered. Hip movements are full.
This technique is done in two cases so fare and the results are encouraging. Due to more roof formation entire head of femur is covered. The hip support is full without any complications
This method is useful in congenital dislocation of hip, development dysplasia of hip, perthe’s disease fracture dislocation hip, old unreduced hip dislocation, proximally migrated head of femur, poliomyelities, failed Salter’s or staheli or pemberton’s surgeries, etc.
3. A prospective study of surgical management of club foot – comparision between suturing vs non-suturing of ‘z’ plasty tendon lengthening.
Dr. Durga Nagaraju, Dr. Ajoy Prasad Shetty, Dr. S. Rajasekaran
Ganga Hospital, Coimbatore.
Relapse of deformity in clubfoot is commonly due to contracture and tethering of the lengthened tendons. Tendon suturing under tension and scar formation at the site of suturing leads to contracture. In infants good healing of tendons without suturing is well known. Elongation of tendons by Z plasty and placing them in good apposition without suturing, with food in corrected position, allows tendons to find proper tension.
MATERIALS AND METHODS:Between January to November 2001, 28 children (age 3 – 12 months) with 44 clubfeet were treated. Two lost for follow-up. Remaining (26 with 41 feet) divided into right side clubfoot (n24) to group A (tendons not sutured after Z plasty) and left side (n17) to group B (Z plasty and suturing performed). All underwent modified TURCO’S poster medial release which included Z lengthening of Tendoachillis, TP, FHL & FDL tendons with posterior capsulotomy of ankle subtalar joint with tenotomy of abductor hallucis and plantar fascia. Both groups evaluated at one year by DIMEGLIO method.
RESULTS:Analyzed results show no significant difference in outcome of the two groups after treatment. Overall results were good in 85.7% children. Preoperatively equinus was the severe deformity followed by varus, adduction and Calcaneo-forefoot rotation (CFF) in both groups. Postoperatively equinus correction was the best than others. Average Dimeglio preoperative score in-group A and B were 10.54 and 10.51, postoperative scores were 3.97 ad 3.91 respectively (p=insignificant). We had 6 feet with residual deformities. Four in group A and Two in group B.
DISCUSSION AND CONCLUSION:Contracture of muscles, due to suturing of tendons under tension, is one of the commonest cause of relapse. Elongating tendons by Z plasty and allowing them to find their own length reduces the incidence of relapse. This study shows there is no particular disadvantage of not suturing the tendons.
4. Revision surgery for congenital dislocation of hip
Dr. Farokh Wadia, Dr. Suraj Gurav, Dr. Tushar Agrawal, Dr. Ajay Hedge, Dr. A.N. Johari
INTRODUCTION:The purpose of this study was to retrospectively analyze the causes for failure of previous surgeries for CDH and to study the complexities of tackling these hips surgically.
MATERIAL AND METHODS:10 Female patients (10 hips) presented to us at an average age of 3 yrs 2 months with unsuccessful previous surgeries done at an average age of 1 yr 7 months. All these patients were evaluated clinically by limb length discrepancy, lurch, and range of motion; and radiologically by Acetabular index, neck-shaft angle. CE angle and Reimer’s index in old, present and post-op follow up X-rays. All patients had a non-concentric reduction after the previous surgery and a dislocated hip in the post-spica X-rays. 3 hips showed AVN on plain X-rays.
We carried out a combination of surgical procedures on each patient after identifying the correct pathology responsible for failure by adequate pre-operative planning on X-rays, MRI and /or CT-scans. We evaluated our results clinically by Modified McKay’s criteria and radiologically by Severin’s classification at 15 months average follow-up.
OBSERVATIONS AND RESULTS:The most common pathology was dense adhesions between the capsule and the femoral head, tight capsule posteriorly and inferiorly and abundant pulvinar and inverted labrum. Bony changes included excessive ante version of the femoral head or of the acetabulum, shallow acetabulum and head-acetabular diameter mismatch. These findings reveal:
- Inadequate OR in the first sitting
- Bony pathologies were uncorrected, e.g. Ante version of femoral neck.
- Large pressure between femoral head and acetabulum due to unyielding soft tissue contracture which should have been tackled by shortening.
It is thus necessary to identify the correct pathology of CDH primarily and get it right the first time, as revision surgeries on these hips are difficult.
5. Role of operative intervention and instrumentation in congenital scoliosis
Dr. Ajay Hegde, Dr Tushar Agrawal, Dr. Farokh Wadia, Dr. A.N. Johari
Historical background and Purpose:Congenital scoliosis is probably the most complex of all spinal deformities to manage. This study highlights the need for timely surgical intervention, with emphasis on role of instrumentation to obtain and maintain curve correction, and adequate fusion preventing progression and worsening of deformity.
Clinical Methods:24 patients underwent surgery for progressive congenital scoliosis from 1997 to 2001. The average age at surgery was 8 yrs 6 months (range: 1 year 2 months- 21 yrs). Most patients underwent anterior and posterior release with fusion with posterior instrumentation (67%). Most commonly used instrumentation is CD: M-8 (77.2%). 2 patients were uninstrumented. Neurosurgery was required in 18.5%.
Results And Follow-up: Average follow-up is of 24 months
Average Cobb’s angles reduced from pre-op of 71.70 (39°– 112°) to postop 53.5° (8-72) resulting in correction of 25.4%
Average kyphosis was reduced from pre-op of 51.8° (20-90) to postop 30.4°
(0-84) resulting in correction of 41.4%.
Complications include infection in 2 patients, hook cut out in 1 patients and transient neuro deficit in 1 patient.
Good fusion mass was achieved in 6 months. There was negligible loss of correction seen in the following period.
Documented progression in congenital scoliosis requires aggressive management irrespective of age. Limited shot segment fusion may suffice in the younger child but multisegment fixation with extensive fusion is required in the older patients. Whenever possible instrumentation should be used to achieve and maintain curve correction and stronger fusion. Pre operative MRI scans are must and neurosurgical intervention may be required simultaneously. The surgery is technically demanding and requires tremendous understanding of the pathoanatomy and instrumentation.
6. Simultaneous anterior and posterior surgery with instrumentation in congenital scoliosis via a single incision in a single sitting (A.p.s.i.)
Dr. A. N. Johari, Dr. Tushar Agrawal, Dr. Farokh Wadia, Dr. Ajay Hegde
Historical background and purpose:Staged or simultaneous anterior with posterior fusion is the accepted treatment in most patients with congenital scoliosis. In all patients the goal of treatment would be to stop curve progression but if partial correction can be safely obtained, it is of additional benefit. This study describes a hitherto undescribed, altogether new approach for simultaneous anterior and posterior corrective surgery via a single incision (A.P.S.I.)
Clinical methods:8 patients underwent A.P.S.I. from 1995 to 2002. Average age at surgery was 4Y 11M and the average follow up period was 24 months. 6 patients had scoliosis and 2 had kyphoscoliosis. 5 had multiple convex hemi vertebrae with unsegmented bar, 2 had multiple convex hemivertebrae and 1 had a solitary hemivertebra. This approach requires a modified thoracotomy incision allowing simultaneous anterior and posterior access to the spine. 6 patients were instrumented (CD-H: 4, Moss Miami:1, Luque:1). Post-op plaster jacket was maintained for an average of 6 months.
Results and follow-up:Average post-op Cobb’s angle required to 85.90 (42-720) from an average pre-op Cobb’s angle of 71.70 (51-900), resulting in an average correction of 17.8%. Average post-op kyphosis reduced to 360 (10-520) from an average pre-op kyphosis of 63.80 (50-950), resulting in an average correction of 43%. At the time of last follow-up one patient (uninstrumented) had an increase in curve magnitude due to pending of the fusion mass.
Conclusions:A.P.S.I. is an excellent approach, well tolerated by the patients allowing extensive and simultaneous anterior and posterior surgery with instrumentation. It saves the patient an additional surgery decreasing the total operative time and period of post-op recovery. This approach can also be used for other pathologies of the paediatric spine e.g. tubercular, pyogenic or neoplastic, to simultaneously execute anterior and posterior procedures.
7. Congenital posteormedial bowing of the tibia
Dr. Alaric Aroojis, Dr. A.N. Johari, Dr. Tushar Agarwal, Dr. Farokh Wadra.
Children’s Orthopaedic Centre and Johari Nursing Home, Mumbai, India.
Congenital posteromedial bowing of the tibia (PMBT) is commonly considered a benign condition with spontaneous resolution occurring in most cases. The purpose of this study is to review our experience with the conservative and surgical treatment of PMBT.
PATIENTS & METHODS:17 out of 26 children with PMBT treated between 1991-2001 were reviewed. Two groups of patients were identified - Group I. Patients who underwent conservative treatment including observation, serial casting or splintage. Group II Patients who underwent correction of residual bowing and leg length discrepancy by osteotomy and limb lengthening using the Ilizarov external fixator.
Results:Group I – 12 patients, follow-up 4.2 years (1 year – 11.5 years) Six patients underwent serial plasters to correct severe calcaneovalgus deformity. The medial angulation was 420 (250 – 580) and posterior angulation was 490 (290 – 700) at presentation, which resolved to 200 (20 – 420) and 190 (00 – 420) at final review respectively. Limb length discrepancy (LLD) was 1.4cm (0.8-2.4cm) at presentation, which progressively increased to 2.6cm (1.5-3.8 cm) at final review).
Group II – 5 patients, follow-up 2.4 years (2 years - 4.5 years). The medial bowing was 210 (120 – 420) posterior bowing was 290 (120 – 420) and LLD was 4.02 cm (3.2 cm - 5 cm) at the time of surgery. The medial angulation was 60 (00 – 100), posterior angulation was 60 (00-100) and lengthening achieved was 6.1cm (5.0 – 7.5cm) at final follow-up. Problems were faced in all five patients during lengthening and included valgus malalignment in four patients, fracture through consolidate in two patients, and additional soft-tissue procedures in two patients.
Conclusion:A large number of patients with PMBT respond to conservation treatment with subsequent LLD being the only sequel. There is a strong correlation between the severity of initial deformity and subsequent LLD. This is the first study to report the results of corrective osteotomy combined with leg lengthening in children with PMBT. Limb reconstruction in this group is a challenge and the risk of complications is high.
8. Arthrogryposis – classification and principles of management
Dr. Alaric Aroojis, Dr. S. Jay Kumar
Alfred I. Dupont Hospital for children, Wilmington, De, USA
Arthrogryposis is a generic term for any disorder presenting with multiple congenital contractures. The purpose of this study was to formulate a classification of arthrogryposis that would be useful to the orthopaedist in making treatment decisions and reporting results.
Methods:220 patients treated at the Arthrogryposis Clinic of our institution from 1975- 2000 were classified into five groups. Group I had amyoplasia or “classic arthrogryposis”, Group II had distal arthrogryposis (Type I and IIA_E), Group III had a specific syndrome diagnosis such as Freeman –Sheldon or multiple pterygium syndromes, etc, Group IV had significant systematic or neurologic involvement, while Group V had unclassifiable contracture syndrome. Birth history, family history, ambulatory status, prevalence of various joint contractures and response to conservative and surgical treatment were studied in each group.
Results:There were 111 males and 109 females (1:1). The average follow-up was 8.2 years (2-24.5 years). Abnormal birth presentations were seen in 37% and Caesarean section was required in 60%. There were 114 children in Group I (65%), 24 in Group II (11%), 13 in Group III (6%), 18 in Group IV (8%) and 21 children in Group V (10%). Group I patients had extensive quadrimelic involvement (83%) with hips involved in 62%, knees in 85% and foot deformity 85%. The commonest foot deformity was equinus or equinovarus. The Upper limbs were involved in ~ 70%. Recurrences were common following surgical release and deformities were usually resistant to treatment. However, at follow-up, 67% were independent or functional ambulators. Group II patients had distal involvement of mainly the feet and hands. Inheritance was autosomal dominant and 33% had affected family members. The deformities were very responsive to treatment and all patients were independent ambulators at follow-up. Group III patients had more sever involvement of the hips in 46%, knees in 70% and feet in 54%, 30% had vertical talus which responded poorly to treatment. Most patients were wheel chair –dependent (54%) and few were limited ambulators. Group IV had severe systemic and neurological problems. These were sick children and mostly bed-ridden. Hips, knees and feet were involved in >90%. Treatment options were limited and morbidity was high in this group. Group V had unclassifiable contractures and generally responded well to treatment.
Conclusion:It is important to classify arthrogryposis since the natural history, extent of involvement and outcome of conservative or surgical treatment are markedly different in the various groups. Proper classification at presentation helps in long-term prognosis and in formulating a rational treatment plan.
9. Management of development dyslasia of the hip in the newborn and infants with the “knee slints” – our experience
Senthil Kumar G.N. Gopal Rathinam, V. Thulasi Raman, Prof., V. Ardhanari
Department of Paediatric Orthopaedics, ICH & HC, Egmore, Chennai
The successful outcome of conservatively Managed dislocation of the hip depends upon an early diagnosis by an accurate screening of all infant and appropriate splintage if instability of hip can be demonstrated. This has been made easy, reliable with the usefulness of the USG of the hip.
The first step in the Management of DDH is closed reduction of the hip, followed by maintenance of the reduction dynamically in a physiologic position. Though Pavlik Harness is being used with success, we in our institution, use knee splints for the maintenance of reduction.
In ICH & HC, Egmore, for the past three years Sep 99- Sep 2003, we have been treating the neonates and infants with this method of splinting with good success. This method is very useful especially in a country like ours, where the patients of low socio economic group, patients with poor compliance, patients from remote areas who cannot turn up for frequent follow up can get good functional out come.
In this paper we analysed the results of 77 cases of developmental dysplasia at the hip (typical) treated by knee splints. The application technique, complications are dealt with.
10. Percutaneous osteotomy for developmental genu valgum
Dr. Swapnil M. Keny, Dr. Taral V. Nagda
Introduction:We describe our experience with percutaneous dome osteotomy for correction of developmental genu valgum.
MATERIAL:Twelve osteotomies were carried out in eight patients with developmental genu valgum with mean age 13.3 years (10-18). The preoperative mean tibio-femoral angle was 23 degree (15-30).
METHOD:Preoperative planning was done on CT scanogram or Full length X-rays. A K- wire is inserted at CORA. Using a specially developed guide multiple drill holes are made to create a dome osteotomy through a single stab incision. The osteotomy is completed using an osteotomy guide. Correction and translation is checked on image intensifier and intra-operative x-rays. The osteotomy is fixed with two cross K-wires and well-moulded AK POP applied. The POP was changed at 2 weeks and maintained for 4 more weeks.
RESULTS:The Mean follow-up is 6 months (2 months to 14 months). The mean tibio- femoral angle immediate postoperative was 6.2 degrees (4 to 10) and 6.5 (3.5 to 10) at the last follow-up. Average loss of correction was 3 to +4 degrees. All patients had full range of knee movements at the last follow-up. MAD was 6 to 10 mm.
CONCLUSION:Percutaneous dome osteotomy provides a simple, precise and cosmetic alternative for correction of developmental genu valgum.
11. Management of rigid and neglected cases of CTEV by JESS – a midterm analysis
Prof. S.S. Gill
PGIMER, Chandigarh
Last decade saw the emergence of external fixaters with distraction capabilities (e.g. Iliazarov, JESS) as an alternative treatment modalities for the rigid and neglected cases of CTEV. JESS has the advantage of locally availability at affordable price and technical case. The present prospective study was done on 43 feet of 41 patients (20 neglected and 23 rigid variety). The mean age of application was 44 months (range 1.5 years to 10 years). No additional bony or soft tissue procedure was done during application. The follow up period ranged from 3.5 years to 6.4 years (mean 58 months).
The final assessment was made according to Lehman –after functional rating system. There were 85% excellent to good results, 13% fair results and 2% poor results. The main complication were temporary oedema (30 feet), pin tract infection (10 feet) and residual forefoot adduction (10 feet).
CONCLUSION:JESS fixator is a good alternative to extensive bony and soft tissue procedures for a rigid and neglected cases of CTEV.
12. Torsional deformities in conservatively treated closed fracture shaft femur in children
Dr. S.S. Gill
30 children between the ages of 11/2 years to 12 years (mean 6.5 years) who sustained fracture shaft femur were treated conservatively and follow up. Assessment of torsion was done by using CT after six months post injury. A significant torsional deformity (>200 difference from the other uninjured side) was observed in 30% of patients. This was independent of variables such as age, sex, type, level and communication of fracture. Those patients with significant increase in anteversion had increased internal rotation and corresponding reduction in external rotation. No gait abnormalities were noticed in any of these patients.
13. Quantitative evaluation of the physical quality of life in Indian children with juvenile rheumatoid arthritis
Dr. S.S. Gill, Dr. Venugopal, Dr. Dhillon MS, Dr. Surgit Singh,
Dept of Orthopaedics, Dept of Pediatric Rhematology & Immunology PGIMER, Chandigarh
Juvenile rheumatoid arthritis is a crippling disease of the childhood. Lot of attention has been focused on the amount of disability caused by this disorder in the western population but no much of attention has been paid to this aspect in the India population. This study quantifies the disability associated with JRA and also quantifies the physical quality of life in Indian patients. In this prospective cross-sectional study with JRA and also quantifies the physical quality of life in Indian patients. In this prospective cross-sectional study conducted in the department of the Orthopaedics in conjunction with department of Pediatric Rheumatology and Immunology, 50 children with JRA who have diagnosed previously and are in follow-up in the department of Pediatric Rheumatology and Immunology, PGI were analysed and the disability quantified using modified Standford health assessment questionnaire and the physical quality of life assessed by a questionnaire, the validity of which has already been tested in the department of Pediatric Rheumatology and Immunology. This study revealed by quantitative measurements, that disability is more in polyarticular type and in those cases in which knee is involved. This study also established quantitatively that activity component of the life is more affected and the grip component is the lease affected in Indian patients with rheumatoid arthritis.
14. The effect of hip adductor muscle release with partial obturator neurectomy on gross motor function in cerebral palsy.
Dr. H.S. Oberoi. M.S., F.C.P.S., Dip. N. B., Raju Sharma B.P.T., M.S.P.T.
Basant Memorial Trust, Oberio Hospital
8 Gujarat Nagar, Jalandhar, Punjab.
The effect of hip adductor muscle release (tenotomy) with partial obturator neurectomy on gross motor function in patients with Cerebral Palsy (spastic) were examined by GMFM (Gross motor function measure).
26 subjects (20 males, 6 females), 15 spastic diplegics, 11 quadriplegia, mean age 12 years, were examined for spasticity by modified Ashworth scale and GMFM was done. After Adductor release & Partial Obturator Neurectomy patients were immobilized in hip abduction, knee extension & ankle in neutral position for 21 days. Physiotheraphy was started thereafter. GMFM was examined 2,4,10 & 14 months after operation.
A decrease in mean GMFM score from 58% to 51% was observed during the first 2 months. It then recovered to 59% at 4 months and thereafter continued to increase. A critical improvement was obtained in 10 cases at 14 months with regular therapeutic exercises.
15. Double Rush rodding in osteogenesis imperfecta-A cost-effective alternative to telescoping rodding.
Gleeson Rebello MS Orth, Benjamin Joseph MS Orth., MCh Orth.
Paediatric Orthopaedic Service
Kasturba Medical College, MANIPAL.
To evaluate the role of double Rush rodding as a cost-effective alternative to telescoping rodding in the management of femoral deformities in osteogenesis imperfecta, and provide a detailed description of the technique.
Methods:Twelve children who underwent double Rush rodding in seventeen femoral segments were followed up over an average of two years. The growth of the rodded femora was measured and the reciprocal migration of the Rush rods was computed from sequential X-rays. The re-operation rate and the complications that occurred with this technique were noted.
Results:The growth of the femora ranged from 7 to 64 mm (median of 33mm). The reciprocal migration of the double Rush rod system ranged from 2mm to 59mm (median of 26mm). Rod migration from the trochanteric entry point occurred in 5 femora and the distance from 7 to 22 mm (median of 14mm).
Conclusion:Though it is technically demanding, double Rush rodding is a cost-effective alternative to telescoping rodding in the management of femoral deformities in osteogenesis imperfecta with a comparable rate of re-operations and complications.
16. Cincinnati incision (modified) to effectively address the postero-lateral tether in clubfoot – my experience
Dr. Ramani Narasimhan
New Delhi
To highlight the effectiveness of a suitable transverse incision (modified Cincinnati) in order to achieve an effective subtalar release in surgical management of CTEV.
Materials & methods:Thirteen patients and 17 feet (4 with bilateral CTEV), who were opened by the author at Indraprastha, Apollo Hospital, New Delhi, between January 1999 and June 2001 have been considered. All deformities were rigid and had been subjected to serial manipulations and casts prior. The surgery was performed in all patients between 4 months and 8 months of age. During surgery, a modified Cincinnati incision was used. Complete subtalar release was done in all, and both talo-navicular and talo-calcaneal joints were reduced and fixed. Sutures were removed after 3 weeks and wires were removed after 6. Full-time CTEV splints replaced casts and subsequently CTEV shoes were added when child walked. All children have a follow-up of 1 & a ½ years at least.
Results:Fifteen out of 17 feet have maintained correction and have satisfactory radiological parameters in the last follow-up. These patients have remained asymptomatic and part from their toddler gait, had a heel-toe gait pattern. Two feet affecting 2 patients, I in a unilateral case and the other in a bilateral case, did not show satisfactory result.
Conclusions:Effective talar mobilization, addressing the postero-lateral tight structures especially, is necessary in order to achieve satisfactory T-N & T-C reduction, in surgical management of rigid CTEV. Although no comparative study has been done, the author feels that a suitable transverse incision (modified Cincinnati) scores over the popular Turco incision in being more cosmetic and more importantly, offering an adequate exposure, which is very necessary for sub-talar release. Slight modification in Cincinnati incision overcomes the problem faced in reaching the musculotendinous junction of gastro-soleus. Proper operative technique & post-operative protocol lessens the probability of posterior skin sloughing.
17. Analysis of footprints of the JESS fixator managed clubfeet
Dr. S. Suresh
Dept. Orthopaedic Surgery, St. Stephen’s Hospital, & Dr. Abrar Ahmed, Dept. of Orthopaedics, AIIMS, New Delhi.
The purpose of the study was to analyze the footprints and report our preliminary short term results of children with Idiopathic Clubfeet managed by JESS fixator which is a relatively newer modality of treatment of clubfeet. Since costly Pedobarograph machines and Gate analysis machines are not universally available, thus simple technique is described as an easy, cheap and reproducible way of analyzing clubfeet managed by JESS fixator.
Materials & Methods:50 feet of consecutive ambulant patients with unilateral clubfoot in the age group of 1-6 years were taken up for the study between January 1998 and December 1999, presenting to Central Institute of Orthopaedic, Safdurjung Hospital, New Delhi. However, at final follow up only 35 patients could be evaluated, whose results are presented here. 14 were dropouts of conservative treatment, 16 were untreated (neglected) clubfeet and 5 were recurrences after previous soft-issue surgery.
Pre-operative & post-operative:Weight bearing footprints of both affected and normal foot (control), were taken. Three months follow up prints were taken post operatively. All patients were managed with JESS fixator. Various parameters like length of footprint, area and pattern, and percentage change from normal foot at the last follow up were taken into consideration vis-à-vis the normal foot which served as a control. Based on footprints appearance grading was done from Grade 1(severely affected) to Grade5 (nearly normal appearing footprint).
Observation & Results:Follow up revealed the achievement of correction in terms of a near normal length, area of weight bearing and appearance in the JESS treated clubfoot to be almost the same as the control foot in approximately 91.4% of the patients (32 out of 25 feet).
Conclusions:The initial results based on weight bearing footprint analysis of the JESS treated clubfeet appear very encouraging, as far as maintenance of cosmesis, foot length and area of contact are concerned. However, the number of patients and the duration of follow-up are less to draw any conclusions. Only a long-term study in a larger subset of patients will reveal how the “Growing” JESS treated clubfoot behaves.
18. Double osteotomy-supracondoylar femoral & upper end tibia for hand on knee gait inpost polio paralysis
Dr. Bhasker Banerjee
Introduction:Hand on thigh gait due to Post Polio Residual Paralysis is a disabling condition. A double Osteotomy-extension Supracondylar Femoral Osteotomy and a second posterior open wedge high Tibial Osteotomy as a single stage procedure has been attempted with encouraging results.
Material & Method:12 cases of Post Polio Residual Paralysis with hand on thigh gait in the age group between 6 to 12 years were subject to this procedure & followed up for a period varying between 24 to 36 months. The cases of hand on thigh gait, which were operated had mild flexion deformities at the knee with Quadriceps power 2 or less (MRC grading) or Quadriceps power 2 or less without any available knee flexor for tendon transfer or unilateral flail knee. All cases undertaken had bilateral stable Hip.
Results:8 cases were able to ambulate without hand on thigh and without external appliances. The other parameters were forward trunk bending, distance in meters they could walk comfortable, lack of posterior knee pain.
Discussion:The advantage of the above procedure over conventional femoral recurvatum osteotomy with patella bone block were.
- Anatomical configuration of articular surface maintained to a greater extent.
- Patella not removed from anatomical site.
- Surrounding ligamentous structure rendered more taut.
- Recurvatum does not increase due to Tibial surface getting posterior inclination.
- Procedure is single stage.
Correcting till of tibia in mediolateral direction is difficult in single stage. Varus deformity is a common problem.
19. Bilateral simultaneous Tibia Lengthening with our without deformity correction in patients with short stature using ilizarov technique: A study of 18 patients.
Dr. Santosh Mathew, M.S., Dr. Hae-Ryeong Song, MD, PhD
Gyeong-Sang National University Hospital, 90 Chilam-Dong, Chinju, South Korea.
Ilizarov coined the term distraction osteogenesis to describe to induction of new bone formation between osseous surfaces that were gradually pulled apart. In our country pathological short stature patients face social, psychological, and physical obstacles in performance of daily activities. This study was performed to determine the safety and effectiveness of performing bilateral simultaneous tibia lengthening with or without deformity correction using distraction osteogenesis in-patients with shot stature due to various causes.
Patients and methods:We reviewed the charts and x-rays of 18 consecutive patients (9 females and 9 males) with 36 tibial segments who underwent this procedure during the period June 1990 to February 2002 in this institution. The average age at surgery was 17.8 years (range 7-28 years). The diagnosis was Achondroplasia in 6 patients, familial short stature in 7 patients, Vitamin D resistant rickets in 3 patients, Spondyloepiphyseal dysplasia in 1 patient, and Turner’s syndrome in 1 patient. There were 6 children (skeletally immature) and 12 adults. There were 19 limbs with marked deformities and 17 limbs without deformities. In all limbs we performed proximal tibial corticotomy for gradual lengthening and deformity correction and stabilized with standard ilizarov frame. Lengthening over nail was done in 13 limbs. In addition 10 limbs had distal tibial osteotomy for acute correction of distal deformity. We also did prophylactic common peroneal release in 12 limbs with deformities. The distraction gap, healing index, external fixation index, and complications were evaluated. The bone result and functional result were also evaluated.
Results:The mean lengthening in 36 tibial segments (distraction gap DG) was 6.59 cm (range 2.5 – 11.2 cm) and the mean lengthening percentage was 28% (range 11.3% to 65.8 The average external fixation index (EFI) in 36 tibial segments was 27.2 days per cm (range 13.4 -58.4). The EFI in nailing group was 30.35 days per cm and non-nailing group was 23 days per cm. Majority of our patients had angular deformity resulting in abnormal mechanical axes preoperatively. A neutral mechanical axis (MAD 0-17mm) was achieved in 29 limbs and 17-20 mm in 4 limbs. Five limbs had persistent MAD of more than 20mm. The mean healing index (HI) was 42.25 days per cm (range 20 – 111.2 days per cm). The mean HI in achondroplasia was 32.15, short stature 45.39, and rickets 68.34 days per cm respectively which was statistically significant (P(<)0.05). There were a total of 73 complications out of which 62 were problems, 3 obstacles, and 8 true complications. Out of 8 true major complications 4 had significant residual deformity, 2 had residual stiffness, one deep infection and one peroneal nerve palsy. The bone result was excellent in 23 limbs, good in 1, fair in 8, and poor in 4. The functional results were excellent in 25 limbs, good in 1, fair in 8, and poor in 2 limbs.
Conclusion:The complexity and difficulty of lengthening and deformity correction in short stature are known to correlate with high complication rates specially if bilateral lengthening is attempting. This study reveals that the simultaneous bilateral tibia lengthening can be carried out without abnormally increasing the complications if prophylactic peroneal nerve release and lengthening over nail is attempted.
20. Bilateral Septic Arthritis of Hips in Neonates
Dr. Vijay Narasimhan, Dr. Vijay Sriram, Prof. K. Sriram
Chennai, Tamil Nadu
Septic hips in neonates are a well-known entity. Bilateral septic hips are not so common. In the last 1 year, 5 neonates with bilateral simultaneous septic hips were treated. 3 cases treated elsewhere with a long-term follow-up are also presented.
Material and Method:The neonates were referred from other hospitals at birth. The neonatologist on clinical suspicion of septic arthritis referred these neonates to us. A focus of infection was usually present. The diagnosis was based on clinical, laboratory investigations and aspiration of the involved hips. The neonates had pseudoparalysis and pain on handling. The hips were gross flexion, abduction and external rotation. The CRP was elevated in all cases. Ultrasound was not relied upon to make a definitive diagnosis. All patients were operated within 2-6 hours after the referral. Cefotaxime and Amikacin were started prior to surgery and then depending on the sensitivity report the antibiotics were altered. Parenteral antibiotics were administered for 10-14 days followed by oral antibiotics for another 4 weeks. Immobilizations of the hips in bilateral spicas was for 3 weeks followed by active mobilization. Of these 8 cases only one child was immunocompromised.
Results:The commonest organism was Klebsiella. One of the neonates died 17 days following arthrotomies. The cause was necrotizing enterocolitis. The other four children had stable hips at the time of discharge. In the three cases treated elsewhere one child had subluxating hips for which bilateral varus derotation oesteotomies have been done. Another child did not have an arthrotomy and has bilateral coxa vara. The third child had unstable hips, which required open reduction.
Discussion and conclusion:The emphasis of this paper is on the need for a high index of suspicion for bilateral septic arthritis in neonates with septicemia. Emergency arthrotomy is the treatment of choice along with appropriate antibiotics.
21. Deformity correction in children by ilizarov method
Dr. R.H. Govardhan, Prof. K. Sriram, Dr. K. Vijayaraj
Department of Orthopaedics, Madras Medical College, Chennai, India
Angular deformities of the upper and lower extremities are common in children following trauma, osteomyelitis and tumourous conditions. The deformity by Malalignment test as described by Dror Paley and correction can be achieved precisely with Ilizarov fixator.
Material:The study was conducted at Govt. General Hospital between the years 1994 and 2002. 23 limb segments were corrected in 18 patients and 10 were males and 8 were females. Age group was from 4 to 17 years with a mean of 10.7 years. Femoral deformity was found in 9, tibial deformity in 7, humeral deformity in 4 and forearm deformity in 3. The aetiology was post-osteomyelitic sequelae in 8, post-traumatic in 5 and one each of multiple ecchondroma, angiomatous lesion, osteogenesis imperfecta and congenital rickets. The LLD ranged between 3cms and 14cms with mean value of 5.3cms. Deformity correction along was done in 12 bony segments in 9 patients and associated limb length inequality was corrected in rest of 9 patients.
Method:Dome Osteotomy and acute correction was done in 12 limb segments. 8 of them were fixed internally. Gradual correction with Ilizarov apparatus was done in 15 limb segments. The Ilizarov construct consisted of two level fixation proximal and distal to the apex of the deformity whenever possible and hinge was placed at the apex of the deformity.
Results:Accurate correction of the deformity was achieved in 20 limb segments and 2 had sub-optimal correction which was clinically acceptable. One patient developed poor regenerate at the distraction site and ended up with recurrence of the deformity. Functional results were good in 16 patients and in 21 limb segments.
Complications:We encountered pin tract infections in 5 patients which subsided with antibiotic therapy. Transient vascular spasm was noted in one of the acute corrections of the deformity which was promptly detected in immediately post-operative period. This was managed by undoing the correction achieved and the deformity was later corrected gradually. Poor regenerate was noted in one patient. Transient peroneal nerve palsy was noted in 2 patients which recovered fully.
Discussion and Conclusion:The Malalignment test of Dror Paley helps in localizing the apex of the deformity and paves way for the accurate correction. Ilizarov apparatus facilitates post-operative adjustments for the accurate correction of the deformity and helps in equalizing the limb length discrepancy.
22. The complications of elastic stable intramedullary nail fixation of paediatric femoral fractures, and how to avoid them.
Unni G. Narayanan, Joshua E. Hyman, Andrew M. Wainwright, Mercer Rang, Benjamin A. Alman.
The Hospital for Sick Children, University of Toronto, Canada
Elastic stable intramedullary nailing has become a popular method of treating paediatric femoral fractures and has been used at The Hospital for Sick Children since 1995. This study reviews the first 5-year experience at HSC, focusing on the complications of this technique.
Materials & Methods:78 children with 79 femoral fractures (mean age 10.5 years) were treated with titanium elastic (flexible) intramedullary nails from 1995 to 1999. Pathologic fractures and fractures in children with metabolic bone disease were excluded. For the 78 fractures that had complete follow-up (median 10 months) the rates of complications are reported, and the factors associated with specific complications analyzed using multiple logistic regression.
Results:All fractures united (median time of 10 weeks). Forty-five of seventy-eight fractures were associated with some complication. Complications included pain/irritation at the insertion site (41), radiographic malunion (8), refracture (2), transient neurological deficit (2), and superficial wound infection (2). Ten patients required a second operation prior to union. The odds of malunion and /or loss of reduction requiring reoperation were significantly increased with the use of mismatched nails (Odds Ratio=19; p=0.002) and comminution >25% (OR=5.5; p=0.02). The odds of pain at the insertion site were increased with leaving them >10mm prominent from the femur (OR=4.5; p=0.002) or bending the nail ends (p=0.02). All symptomatic nails were removed. Nails remain implanted in 25 children without problems.
Discussion & Conclusions:2/3rd of these fractures were associated with high-energy trauma, which might account for the high rate of complications in this series. Most of these complications are minor, and many are preventable. Nails of two different diameters should not be implanted. Nail ends should not be bent but advanced that they lie against the supracondylar flare of the femur to avoid symptoms at the insertion site. The study questions whether routine elective removal of nails is necessary.
Posters
1. Correction of long-term contracture of wrist in children using Ilizarov
Dr. Veeramanjunath, Dr. Sivaramakrishna, Dr. Vrisha Madhuri
CMC, Vellore
Long-standing contractures are difficult in management problems, especially in the wrist and hand, where there is a paucity of the covering soft tissue. The contracture by soft tissue release is limited by tight neurovascular structures and staged procedure may be need due to poor soft tissue wedging.
We present tow cases of long-standing contracture.The first one is a boy aged 5 years old with burns contracture of the hand and wrist sustained at 6 months of age. He had flexion contracture of the wrist and extension contracture of the MP joints.
This stiffness was corrected by gradual distraction using Ilizarov apparatus. The function of the hand improved significantly. The second was a case of rheumatoid arthritis in 11-year-old male child with 900 flexion deformity of the wrist.
In view of previous experience we decided to treat with Ilizarov. Frame consists of simple 2 rings with hinge at the level of lunate. A distraction rod was applied anteriorly and distraction was carried out and full correction of deformity was obtained. The child was treated with dorsiflexion splint to prevent relapse of the deformity for further period of 6 months.
In both our patients the function and the appearance improved significantly. Though unipolar external fixator are frequently used in hand and forearm. Ilizarov so far has not been popular, so for in wrist deformity. We described these two cases in children to emphasize the simplicity and versatility of this over the other method of correction.
2. Displaced fracture of the distal metaphysis of the radius and ulna with a plastic deformity of the ulna with a milch. Type I fracture of the lateral condyle of the humerus – a case report and a proposed mechanism of injury.
Dr. Keny Swapnil M.
Mumbai
A displaced fracture of the distal metaphysis of the radus and ulna associated with a supracondylar fracture of the humerus is common. However such injuries associated with fractures of the lateral condyle of the humerus have not been reported.
CASE REPORT:A three year old female child presented with a history of fall on the outstretched hand. Examination revealed a swelling over the wrist and elbow joint with a deformity of the forearm. There was no distal neurological deficit. Roentgenograms revealed a dorsally angulated and displaced fracture of the radius and ulna distal metaphysis with a plastic deformity of the middle third of the ulnar with milch type I fracture of the lateral condyle of the humerus.
DISCUSSION:Surgical anatomy – A child’s bone is more flexible because the haversian canals are large and thus render the bone more porous. This allows a greater degree of flexibility and hence more platic deformation to occur before fracture. Chamay showed that low level stress applied to a bone causes bending proportional to the stress applied, but the bone retains its normal configuration when stress is removed. This fixed bending is not associated with gross fracture and is called plastic deformation. Longitudinal compressive forces applied to a naturally curved bone has been shown to cause plastic deformation. Tensile stress is produced at the convex surface and compressive stress occurs at the concave surface. Bending occurs through oblique slip lines. These slip lines extend from the periosteum to the medullary canal at an angle of about 30 degrees to the long axis of the bone.
3. Flexion deformity of the elbow joint due to fibrosis of the bracchioradialis after administration of intravenous fluids in a child – A care report
Keny Swapnil M, Desai M.M
Dept of orthopaedics, KEM Hospital, Mumbai
Contractures of the quadriceps and gluteus maximus have been frequently reported. However a deformity of the elbow due to brachioradialis contracture is not reported.
Case report:A 8 year old male child presented with a 30 degree flexion deformity of the elbow. Following administration of intravenous fluids in the pediatric ward for bacillary dysentery. The parents gave a history of extravasation of the administered fluid and elbow swelling following this administration. On examination there was fibrosis of the brachioradialis with nodule formation in the substance of the muscle. The deformity was partially correctable with stretching under anaesthesia. The patient was administered rigorous physiotherapy for a period of two weeks and the contracture was corrected.
Discussion:extravasation of a intravenous fluid especially a colloid solution can cause a severe inflammatory reaction in the muscle tissues which heals with fibrosis. In children this reaction can be intense causing fibrosis and significant disability.
4. Congenital insensitivity to pain – a variant
Dr Anand Rengasamy
Trichy
Congenital insensitivity to pain is a very rare condition. Various types and subtypes have been described in the literature. I am reporting a case with universal loss of pain sensation loss of heat perception, which has not been reported in the literature.
Congenital Insensitivity to Pain – A Variant:Congenital insensitivity to pain is a rare condition, which may affect various tracts in the peripheral nervous system. In the literature, five types have been described. I am describing a case who has universal loss of pain sensation and a selective loss of heat perception. Other sensory tracts were well preserved. Selective loss only to heat perception could not be explained and has not been reported earlier. This case may be a variant of congenital insensitivity to pain.
5. The Foot in Multiple Synostoses Syndromes
Gleeson Rebello, Benjamin Joseph
Paediatric Orthopaedic Service, Kasturba Medical College, MANIPAL
We studied cases of multiple synostoses syndrome to identify the pattern of tarsal coalition, the foot deformities and procedures employed to make the feet plantigrade.
Methods:Radiographs and case records of four patients with multiple synostoses syndrome treated in over a period of fourteen years were reviewed. The pattern of fusion, the foot deformities and the operations performed were studied.
Observations and results:All four patients with multiple synostoses syndrome had carpal and tarsal coalition and symphalangism. Three of the patients were from one family with an autosomal dominant inheritance pattern. The fourth case appeared to be a sporadic case without a positive family history. Severe inversion of the forefoot and a mild degree of hindfoot varus were the characteristic deformities seen in all the feet. Hindfoot equinus was present in one case. All the deformities were rigid. We performed an external de-rotation osteotomy at the midtarsal level and a lateral displacement osteotomy of the calcaneus, to make the feet plantigrade.
Conclusion:A clear understanding of the pattern of fusion and the characteristics of the deformities should enable the choice of the optimal treatment for improving the foot function in patients with some of these less known conditions like multiple synostoses syndrome.
6. Management of the mirror foot and its associated anomalies
Gleeson Rebello, Benjamin Joseph
Paediatric Orthopaedic Service, Kasturba Medical College, MANIPAL
We document our experience in the treatment of this uncommon form of polydactyly and the impact of associated ipsilateral limb anomalies on its management.
Methods:The treatment of four cases of mirror foot was reviewed. Ipsilateral limb anomalies were documented and their bearing on the management of this condition was analyzed.
Observations and results:The associated musculoskeletal anomalies seen were developmental dysplasia of the hip, fibular dimelia and tibial hemimelia. The surgical procedures were aimed at treating the associated conditions before ablating the extra rays to improve the cosmetic appearance of the feet. The intactness of the quadriceps mechanism was a key factor that guided the preservation of the knee joint and the anomalous limb distal to it. In one case the hip was contained prior to treating the mirror foot. In three cases we reconstructed the quadriceps mechanism. We also had to correct the severe equinus at the ankle joint and stabilize it before treating the mirror foot. We used an orthosis in one child to stabilize the knee and make the foot plantigrade.
Conclusion:There are few reports in the literature on the surgical management of this rate condition and its associated anomalies. If correction of associated deformities is performed using the right principles and in the appropriate sequence, it may be possible to avoid an amputation.
7. Clinico radiological evaluation of perthe’s disease
Dr Gill S.S. Dr. Ravishankar M.R., Dr. Dhillon MS Dr (Mrs.) Katariya S.,
PGIMER, Chandigarh
Leg-Calve-Perthe’s Disease (LPCD) is an idiopathic avascular necrosis of the femoral capital epiphysis and its resulting sequelae usually occurring in the children in the first decade of life. The disease being self healing and the pathology involving the femoral head, the main objective of the treatment is to obtain a spherical head as the final outcome.
The purpose of the study is to assess the sphericity of the femoral head in the LCPD by plain radiography and to correlate it with the functional range of movement of the hip joint.
Keeping in the Indian context where the expensive investigations like Arthography (investigation of choice), CT, MRI, are routinely not available for assessing the sphericity of the head at all levels of health care management because of the limited resources. This study utilized X-ray as a tool for assessing the sphericity.
Methods and materials:Patient of all age group and both sexes are included in the study. Patients are assessed for active range of movements in the supine position. Movements are particularly examined for flexion, abduction, internal rotation, which are mainly affected in LCPD. Movements are measured by goniometer. Movements are classified as food, fair and poor categories. Ap and lateral view X-ray are taken the sphericity of the affected hip measure by Mose’s tamplate. Sphericity is classified into good, fair and poor categories. Sphericity is correlated with clinical range of movement. Multiple combinations are drawn.
Observations:Out of 30 cases, 10 cases were in the age group of 4-6(53.33%) years. 11 cases are in the age group of 7-9(36.67%). 3 cases are in the age group of 9-12 years (10%). Mean age at presentation is 6-9 years. Male: Female ration was 10:1. Sphericity assessed into 30 patients by Mose’s template
1. Good to fair results were found in 22 out of 30 cases
2. Out of 24 conservatively managed cases had good radiological sphericity and excellent range of movement.
3. 5 out of 6 surgically managed cases had good to fair radiological sphericity and excellent range of movements.
A good spherical head should be the optimum goal, whether managed conservatively or surgically, since it directly affects the functional range of movement of the hip joint. There is not much of significant variation in the functional outcome whether managed conservatively or surgically.
8. Familial hypophoshataemic rickets a case report
Dr. Pramod Mohan, Prof. Gill S.S., Dr. Jain N.K.
Hypophostaemic Vitamin D resistant rickets, one of the common metabolic bone diseases in developed countries and one of the most common causes of dwarfism in orthopaedic clinics, is an X-linked dominant disorder (although sporadic cases also occur). It is characterized by short stature, lower extremities and defective mineralization of bone. While basic biochemical defects vary among involved individuals, all patients show a failure of the proximal tubule of the kidney to resorb inorganic phosphate. Radiographic findings are the same as in vitamin deficient rickets, however in these cases the changes are more marked in the lower limbs particularly around the knee. Laboratory findings consist of low serum phosphorous, elevated alkaline phosphatase and abnormal serum calcium.
Since it is a multidisciplinary problem, these patients are usually followed by a paediatrician or an endocrinologist high doses (as was done in the past) has been found to have little beneficial effect on these lesions. Moreover if not closely supervised, this regimen carries the risk of hypervitaminosis D. today the treatment is done with neutral phosphate orally along with 1.25 dihydroxyvitamin D3.
The deformities encountered mainly by the orthopaedic surgeon are usually in their lower limbs and include genu valgum or varum, anterior angulation of femur, anterolateral angulation of the tibia, coax vara and intrapelvic protrusion of acetabulum; in spine kyphoscoliosis may be problem. Mild deformities correct with supportive foot wear and medical treatment but moderate to severe deformities may require supportive orthotic devices and at times corrective osteotomies. Vitamin D is stopped 4 to 6 weeks prior to surgery to prevent hypercalcemia resulting from cast immobilization and reinstituted once cast is removed and normal activities are resumed. Post operative immobilization is kept to a bare minimum in these patients.
We are presenting 3 families affected with hypophosphataemic rickets with diagnostic problems and their management.
9. Long arm cast in extension for forearm in children
Dr. Alaric Aroojis, Dr. Manoj Singrakhia, Dr. Shantanu Deshpande, Prof. Kaye Wilkins
Kind Edward VII Memorial Hospital, Mumbai, India
To study the efficacy of long arm cast with elbow in extension for treatment of unstable forearm fractures in children.
Patients and Methods:60 consecutive aged < 16 years, presenting to our Trauma Center with displaced or angulated forearm fractures were randomly assigned, after closed reduction under anaesthesia /sedation, to either of 2 groups. Group I: Long arm cast with elbow in flexion; Group II: Long arm cast with elbow in extension. All children were followed up at 1-,2-,4-,8-,12- weeks, 6- and 12 months, clinically and radiologically to note for re-displacement or re-angulation with the cast. Limits of acceptability were set at < 10-150 of angulation and (<)30-450 of malrotation. Elbow ROM and forearm rotations were measured after cast removal and on follow-up.
Results:There were 30 patients in each group and both groups were matched for age, type of fracture and pre-reduction angulation / displacement. After reduction, unacceptable angulation persisted in 3 patients in Group I but none in Group II. At 2- week follow-up, 3 more patients in Group I angulated within the cast and had t be re-manipulated and treated in extension cast till union. A statistically significant number (p(<)0.05) of fractures in Group I developed unacceptable angulation as compared to Group II. All patients had full elbow and forearm motion at 6-months follow-up. Complications included cast slippage in 3 patients in Group I and superficial plaster sore in 1 patient in each group.
Conclusion:The conventional method of treating unstable forearm fractures with the elbow in flexion results in an unacceptable degree of angulation with the cast. As the cast slips distally, the bend at the elbow may actually cause the fracture fragments to angulate further (Rang, Wilkins). Casting with the elbow in extension using the proper technique is and effective and innovative method to avoid angulation during the period of cast immobilization, as has been shown in this pilot study. This technique is superior to alternative methods such as percutaneous intramedullary fixation, plating, or pins and plaster for management of unstable forearm fractures in children.
10. Predictive value of standardized intraoperative radiographic measurements on postoperative residual deformity of club foot.
Dr. Senthil Nathan, Prof. S.S. Gill, Dr. M.S. Dhillon & Dr. Ravi Shankar
PGIMER, Chandigarh
PMSTR is the most common surgical procedure performed on a CTEV foot. Residual deformity following PMSTR is very common problem. Most of the surgeons, use their clinical acumen to asses the adequacy of correction achieved intra operatively. Clinical assessment alone is misleading and erroneous at times. Intra operative radiography as a toll to assess the correction achieved is surrounded by lot of controversies and disbeliefs. No clinical trial has been done so far, to prove or disprove the adequacy of radiography as a tool for assessing the intra operative correction achieved. In our study an attempt has been made to standardize the radiographic technique of CTEV and to chart out a radiographic parameter for each of the deformities of CTEV, and also to assess the extent to which the intra operative radiological correction of the deformities, correlates with the clinical outcome.
Aim:The aim of the study is to assess the predictive value of intra operative radiography as a tool to measure the adequacy of correction achieved intraoperatively for a CTEV foot.
Methods and Materials:In our study 30 TEV cases in the age group 6months to 2 years who underwent PMSTR were preoperatively assessed both clinically and radiographically. Radiography was done using Simon’s Standardized technique and a specially designed splint. Stressed AP and lateral views were taken.
Radiographic values were noted in a special radiographic chart which contains standards radiographic parameters for each of the deformities of foot. Intraoperatively once if the surgeon feels that clinical correction has been achieved, with the wound open, radiography taken according to standards using Simon’s radiographic technique and special sterile splint. Cases were divided into two groups one in which radiological correction is achieved and one in which radiological correction is not achieved. Clinical outcome for each of these groups evaluated using Demeglio’s score and hence the correlation between radiological correction and clinical outcome ascertained using paired test. It was found that group in which radiological correction was achieved had a significant reduction in the incidence of the residual deformity rate as compared to the group in which the radiological correction was not achieved.
Conclusion:From our study, it is evident that intraoperative radiography if well taken and assessed meticulously can predict the residual deformity and hence the clinical outcome in CTEV. Hence, it can be conducted that intra operative radiographic assessment of DTEV foot, if standardized, is a mandatory rather than an optional measure and every child should be provided with an opportunity to be assessed radiographically intraoperatively.
11. Role of corrective serial plaster cast application in management of ctev presenting with moderate delay
Dr. Aril Gul (MS), Dr. S.S. Gill, MS
Department of Orthopaedics, Post graduate Institute of Medical Education and Research, Chandigarh
We studied the influence of serial corrective plaster cost application in CTEV who presented to us between age group 1 and 6 months. All type 1 CTEV which are postural in nature and type 3 CTEV which are secondary to other disorders like arthrogryposis, poliomyelitis, diastrophic dwarfism were excluded from the study. All the patients who were included in the study were evaluated clinically and radiologically before serial casting was begun. Six serial casts were applied at 15 days intervals and after a period of 3 months, they were again evaluated clinically and radiologically.
Serial POP correction is a good option in the treatment of type II-CTEV, in cases presenting with moderate delay. Full correction of the feet in delayed cases is possible by serial casting only in few percentage of cases; however, there is a marked improvement in the various deformities. Except for equinus deformity, which is partially resistant to casting, adduction being most amenable to casting treatment. Since this does not correlate well with the reported literature a longer follow up is recommended to see for relapse of forefoot adduction. The role for percutaneous tenotomy of tendo achilles during casting may be significant and needs to be studied. Cast care throughout the period of casting is essential and the child’s parents need to be motivated about the need for serial casting. An additional finding noted was the good correlation between clinical deformity and radiological parameters in CTEV.
12. Simple bone cysts – Do they heal once fractured?
Dr. Pramod S.
Dept of Orthopaedics, KMC Hospital Attavar, Mangalore.
Simple bone cysts are benign fluid containing lesions, usually expanding in nature and seen in children before skeletal maturity. There are various views regarding the cyst healing after a fracture through the cyst.
We reviewed 15 children who presented after a fracture through a simple bone cyst to investigate the fate of a cyst once framed. 4 patients had fractured through the cyst more than once. All the fractures healed rapidly after non-operative treatment. At a median follow up 1.5 years (range 1 to 4.5 years) one cyst had disappeared spontaneously and one healed following treatment with steroid injections.
We conclude that the natural history of simple bone cyst is not altered by a fracture and probably cyst needs to be treated once the fracture heals.
13. Ilizarov alternative for old unreduced monteggia fracture dislocation
Dr. Sanjay Yadav, Dr. Nitin Modi, Dr. Ashok Rathod, Dr. S.M. Shahane & Dr. R.H. Pathak
R, 10 years old male, presented with right elbow deformity since 1 year, fixed flexion of 6 degrees with further flexion up to 100 degrees X-ray revealed old unreduced Monteggia fracture dislocation with posterolateral dislocation of radial head with dorsolateral angulation of upper third ulna.
Patient treated with upper third osteotomy, acute anterior and medial angulation was given at the osteotomy site and maintained with Ilizrov ring fixator. After 14 days, the osteotomy was distracted for lengthening of ulna and maintaining the angulation till the radial head was brought 4 mm below the level of capitulum. At that stage an olive wire passed from dorsolateral to anteromedial direction into the radial neck and the radial head was gradually pulled into its reduced position and maintained for two months.
Patient’s elbow range of motion improved with extensive physiotherapy. At present no flexion deformity and range from 0 to 120 degrees is present. X-rays at 6 months follow up after removal shows less than 50% subluxation though no posterior subluxation was present. Patient has good pronation and supination and is asymptomatic at one and half year of follow-up.
14.Result-oriented aggressive surgical package in spastic diplegic cp
Ramani Narsimhan, Delhi
Aims/Objectives:To emphasize the importance of anticipating gait problems & planning multiple surgeries over lower limbs in a single GA sitting preferable, in patients of spastic diplegics CP
Materials & Methods:Twelve patients of spastic diplegics CP between 4 years and 10 years of age, who were managed by the author at Indraprastha Apollo Hospitals, New Delhi, between January 1999 and December 2001, have been considered. Seven patients had abnormal independent gait but the other 5 had never walked independently. Gait laboratory facilities being unavailable, regular clinical examination by the author along with the PT, OT and orthotist, supplemented by appropriate radiographs, influenced my decision to plan the surgeries for each patient. Majority was operated between 6 and 8 years of age. Eight patients were subjected to soft tissue procedures alone whereas the other 5 had both soft-tissue and bony procedures. Post-operatively, all patients underwent gait training using appropriate AFOs and also received regular PT & OT. All patients have been followed up for a period of 1 year at least.
Results:All patients improved after surgery and the post-operative protocol. Six out of 7 patients who never walked independently started doing so, whereas I still walk with support. All patients have plantigrade feet while standing, and heel –toe gait.
Conclusion:Spastic diplegics peak with their gait problems between 5 & 8 years of age, and majority require surgical intervention to offer independent gait or improve it. Identifying the offending muscle groups and the bony anomalies responsible, and tackling them all surgically at the same time, would reduce the risks of multiple anaesthesia and more importantly, make the post-operative gait-training and rehabilitative program maximally effective.
Management Options in Congenital Scoliosis
Dr. Ashok N. Johari
M.S. Orth., F.C.P.S., D. Ortho., D.N.B. Ortho.,
M.A.M.S., M.Ch. Orth., England
Hon. Prof. Of Orthopaedics, Grant Medical College
Padiatric Orthopaedic Surgeon,
B J Wadia Hospital for Children,
Sir J J Hospital,
Bombay Hospital,
Lilavati Hospital,
Mumbai, India
Address for communication
Dr. Johari’s Nursing Home
C.S. No. 993, Raj Ratna, Dr. Raikar Marg
Mahim (West), Mumbai 400 016, India.
Email:-drashokjohari@hotmail.om
Fax:091-22-24445599
The five major problems in congenital scoliosis are
- Trunk deformation
- Trunk decompensation
- Truncal shortening
- Altered neurology
- Other congenital anomalies
The major target site for deformation in congenital scoliosis is the vertebral bone itself. It is truly a “bony” scoliosis and principles of bone growth do apply.
1. Trunk deformationArises out of growth imbalance on the two sides of the spine. The reason for this growth imbalance is structural.
- Presence of wedge or hemivertebrae on one side of the spine
- Presence of an unsegmented bony bar with or without contralateral hemivertebrae
The site of the bony anomaly is important as lower thoracic and thoracolumbar curves have a larger propensity to increase. Upper thoracic or cervical scoliosis has a highly visibility and becomes a cosmetic problem much earlier.
The unsegmented bar in combination with contralateral hemivertebrae has the greatest potential for deformation followed by a unilateral unsegmented bar or double / single hemivertebra. Hence it is important to identify the structural defect responsible for the spinal deformity.
2. Truncal decompensationA solitary hemivertebra located strategically may give rise to truncal decompensation. This happens at the junctional zones e.g. the lumbosacral junction (oblique take off), the thoracolumbar or cervicothoracic junction. Large rigid curves may show poor compensation above or below the curve. Trunk balance is an important aspect to be considered in treatment planning.
3. Truncal shorteningDue to reduced growth potential truncal shortening may be visible. Secondarily due to early spinal fusion the truncal height may be reduced. However, a short straight trunk is better than a deformed one. We have currently no means available to increase truncal height and this remains a research area.
4. Altered neurologyCongenital scoliosis is characterized by a high incidence of intraspinal problems ranging upto 30% in some series. These comprise pathologies like those of diastematomyelia, fibrous splitting of the cord, low filum terminal, cord or root tethering etc. These may be responsible for altered neurological treatment signs prior to treatment. They also have important implications for surgical treatment e.g. distraction instrumentation. This may demand rectification of the intraspinal pathology prior or along with the definitive surgical treatment.
5. Other congenital anomaliesThe VATER association and presence of other anomalies e.g. cardiac or genitourinary may have a bearing on treatment and all congenital scoliosis need to be evaluated for presence of other congenital problems.
TREATMENT OPTIONSAge, remaining growth, presence of other congenital defects and neurological status are important in clinical examination. A thorough clinical and radiological evaluation should include analysis of the type and site of vertebral anomaly, trunk balance, presence of laminar defects and signs of occult dysraphism etc.
The treatment options when faced with a patient of congenital scoliosis are either non operative or operative.
1. NON OPERATIVE TREATMENT
1. Observation
Small curves
Initially to determine progression
2. Bracing
Curve < 400 with flexibility of 50%
Where better trunk balance can be obtained by bracing
Post operative management of curves where localized apical fusion is carried out.
Bracing has limited role in congenital scoliosis.
Operative management is indicated for congenital scoliosis in the following situations
- Progressive increase in deformity
- Trunk decompensation
- Neural deficit
The types of surgeries carried out for congenital scoliosis are as follows:
- Prophylactic to prevent progression
- To improve trunk balance
- Salvage- correction of deformity
- Neurosurgery
i. Combined anterior + posterior convex epiphysiodesis
This is a growth arrest procedure which effectively stops growth on the convex side. When growth potential exists on the concave side, some curve correction may be obtained. This is best done for small curves 600 preferable by five years of age.
ii. Posterior /anterior + posterior convex apical fusion increasing curve in an immature patient demands a convex anterior + posterior fusion. This is a limited fusion and requires post operative support and bracing.
The option of subcutaneous rodding of the curve and apical fusion seems largely unacceptable in developing countries because of the frequent surgery required. Growth rods may have a role to play in such a situation.
iii. A progressive deformity in a nearly skeletally mature patient would need correction, posterior fusion and instrumentation to support the fusion. Different options of instrumentation are available with their merits and demerits.
In a similar situation where the deformity is severe and rigid, anterior release needs to be combined with posterior instrumentation and fusion.
The aims of these procedures is to restore spinal balance and not to achieve maximal curve correction.
i. Hemivertebra resection with or without instrumentation
This is indicated where the cause of truncal imbalance is the hemivertebra. This occurs at the junctional zones. The Hemivertebra needs anterior and posterior resection. Where suitable a posterior compression assembly can be used. This surgery can occasionally be carried out by a single posterior approach in which the hemivertebra is exicised from the posterior approach.
The procedure of hemivertebra resection is associated with risks especially in the thoracic region and must be undertaken by an experienced surgeon.
ii. Total vertebrectomy, correction, instrumentation and fusion.
This is reserved for rigid decompensated curves to improve spinal balance and gain correction. It is technically a demanding procedure and should be used for cases which have marked decompensation. The procedure involves anterior resection or decancellation, corresponding posterior resection, instrumentation and fusion.
Correction of the deformity will most often involve the above procedures. In severe curves, anterior surgery is combined with posterior surgery, instrumentation and fusion.
Neurosurgery in congenital scoliosisIn congenital scoliosis the incidence of intraspinal pathology tethering the cord is high. All intraspinal problems do not need active intervention. This is necessary where a spinal dysraphism is symptomatic or likely to become symptomatic or where distraction instrumentation is planned. Rapidly increasing scoliosis should entail a search for intraspinal pathology. Such problems can be dealt with as an isolated procedure or combined with posterior surgery for scoliosis.
TECHNICAL NOTES- All cases of congenital scoliosis should have a MRI to know the cord status, canal diameter and narrowing, intraspinal pathology etc.
- In the thoracic region, limited anterior + posterior surgery e.g. epiphysiodesis or apical fusion can be carried out via a single sloping thoracotomy incision. The incision can be retracted to the mid line for the posterior fusion. I have been using this approach for many years now.
- Instrumentation should be used with caution in cases of congenital scoliosis. A proper assessment of the vertebral size, canal size and age of the patient has to be made. The highest incidence of neural complications of instrumentation exists in this group, Instrumentation can be used without distraction to support the spine. Alternative to this is cast support, wedging and cast correction of the spine.
- Laminar defects may make exposure and instrumentation difficult and alternative sites of purchase like the pedicle and transverse process should be sought in these cases.
- Anterior instrumentation should be avoided in a severely rotated spine.
The biggest error in the management of congenital scoliosis is procrastination in offering surgical management. Prophylactic fusion should be considered for curves which are known for rapid progression e.g. those with unsegmented bar and contralateral hemivertebrae. Progressive curves should be fused regardless of age. Neurosurgical aspects of scoliosis management should not be neglected. Management options should be weighed and considered in each situation.
Abstract
MANAGEMENT OF PAINFUL STIFF HIP IN CHILDREN
Dr. Ashok N. Johari
M.S. Orth., F..P.S., D. Ortho., D.N.B. Orth.,
M.A.M.S., M.Ch.Orth., England
Hon. Prof. Of Orthopaedics,
Grant Medical College
Padiatric Orthopaedic Surgeon,
B J Wadia Hospital for Children,
Sir J J Hospital,
Bombay Hospital,
Lilavati Hospital,
Mumbai, India
Painful or painless stiff hips in children are a problem in management. What causes them and how does one treat them?
Stiff hips are a sequel to the following aetiologies:
- DDH with avascular necrosis or infection complicating treatment
- Slipped capital femoral epiphysis with AVN
- Adolescent Perthes disease
- Post-traumatic AVN
- Septic Arthritis
- Tuberculous or rheumatoid arthritis
- Cerebral palsy
- Skeletal Dysplasia
- Idiopathic chondrolysis
- Latrogenic
The mechanisms by which stiffness occurs are the following:
- Muscle contractures
- Capsular fibrosis and thickening
- Cartilage damage
- Bony incongruity
The management rationale for a painful or painless stiff hip would be
- Establish the diagnosis
- Treat active disease
- Mobilise the joint if pain can be controlled. Rarely immobilization of the joint followed by mobilization may be needed
- Examine the surgical options
The various surgical options for stiff hips in children are:
- Muscle release
- Capsular releases and capsulectomy
- Arthrodiatasis
- Cheilectomy
- Osteotomy – femoral or pelvic
- Arthrodesis
- Arthroscopy and excision of loose fragment (Osteochondritis dissecans) This lecture illustrates the principles of management of a stiff hip.
Management of Short Stature
Dr. P. RAGHUPATHY, MD, DCH, FRCP.
Paediatric Endocrinologist and
Professor of Paediatrics
Christian Medical College, VELLORE
| Diagnosis | Mid parental | Bone age | Predicted adult | HGH | Other |
|---|---|---|---|---|---|
| centile | height | ||||
| Genetic shortness Normal |
Low | Normal | Low-but normal for parental centile | - | |
| Genetic delay | Normal | Delayed | Normal | Normal, but may need repeated test afteroestrogen and androgen priming | - |
| Short / delay | Low | Delayed | Low-but normal for parental centile | Normal, but may need repeated test afteroestrogen and androgen priming | - |
| Partial hGH deficiency | Normal | Delayed | Below parents | Consistently < 20miu/I | |
| Deprivation | Variable | Delayed | In severe cases may be low | Variable, but may be very low. May improve after propranolol (Collu et l 1978) | Improvement clinically and biochemically after separation from home |
| Malabsorption | Normal | Often very delayed | Usually normal for family | May be low | Other signs or symptoms usually present but mild |
Differential diagnosis of short / delay:
| Name | Major clinical features | Major radiological feature | Inheritance | Prognosis |
|---|---|---|---|---|
| Achondroplasia | Rhizomelic short limbs. May not be obvious at birth | Narrow deep sacro iliac notches. Abnormal lumbar vertebrae. Flaring metaphyses | Dominant 80% new mutations | Good |
| Homozygous achondroplasia | More market than achondroplasia. Small thorax | Similar to but more marked than achondroplasia. Spike on lower femur | Both parents have achondroplasia | Neonatal death |
| Achondrogenesis la. Parenti-Fraccaro |
Soft skull but head not enlarged. Extremely short limbs and small thorax | Poor or absent ossification of skull and vertebral bodies. Abnormal ribs – short and thin with possible fractures | Autosomal recessive | Neonatal death |
| 1b. Langer-Saldino | Large head | Gross under-ossification of lumbar vertebrae, sacrum and pelvic bones Sacroiliac notch normal | Autosomal recessive | Neonatal death |
| 2. Grebe disease | Normal head and trunk with very short hypoplastic limbs | Hypoplasia of limb bones. Other bones normal | Autosomal recessive | Good |
| Thanatophoric dwarfism ‘Death seeking’ | Very short extremities and arrow thorax | Similar to achondroplasia but more severe. Lumbar vertebrae have inverted U appearance. Ribs short | Sporadic | Neonatal death |
| Chondrodysplasia punctata | ||||
| 1. Rhizomelic type | Rhizomelic short limbs. Cataracts and metal Retardation | Cartilaginous stippling. Metaphyseal cupping | Autosomal recessive | Most die in infancy |
| 2. Conradi-Hunermann type | Dwarfism not of rhizomelic type | Normal metaphyses | Usually dominant | Reasonably good |
| Metatropic (‘changing’) dwarfism | Short extremities in new born period resembling achondroplasia. In late infancy kyphoscoliosis develops | Platyspondyly. Expanded metaphyses of long bones which resemble dumb-bells. Normal cranium | Autosomal recessive | May die in infancy or survive to adulthood |
| Metatropic type II (Kniest syndrome) | Similar picture with abnormal facies | Vertebrae flat from birth. Maxillary hypoplasia Abnormal epiphyses and metaphyses | Sporadic | Usually survive |
| Disastrophic dwarfism | Short limbs, progressive scoliosis, club feet | Fusion of proximal and middle phalanges. Short wide metacarpals, phalanges and long bones. Abnormal epiphyses | Autosomal recessive | Usually survive |
| Chondro-ectodermal dysplsia (Ellis-van Creveld) | Shortness affects middle and distal segments of limbs, Polydactyly, ectodermal defects and congenital heart disease (ASD) | Short squat distal limb bones with expanded metaphyses. Abnormal pelvis | Autosomal recessive | One-third die in infancy |
| Asphyxiating thoracic dysplasia (Jeune) | Short limbs of varying severity with extremely short ribs | Very short horizontal ribs with expanded costo-chondral junctions. Abnormal dysplasia | Autosomal recessive | Often die in infancy |
| Sondylo-epiphyseal dysplasia congenita | Limbs long in relation to trunk but short compared with normal | Platyspondyly and proximal epiphyseal dysplasia | Autosomal recessive | Usually survive |
| Mesomeli dwarfism | ||||
| 1. Langer type | Generalized shortening of extremities with marked hypoplasia of ulna, fibula and mandible. Ulnar deviation of hands | Hypoplasia of ulna and fibula, humerus nd femur | Autosomal recessive | Good |
| 2. Nievergelt type | Very short forearms and shanks with deformed elbows. Rest of skeleton normal | Very short deformed radius and ulna, tibia and fibula | Autosomal recessive | Good |
| Acromesomelic dwarfism | Marked shortening of forearms, hand and feet | Radius bent and ulna very short. Metacarpals, metatarsals and phalanges very short | Autosomal recessive | Good |
| Cleidocranial dysplasia | Mild shortness with maldevelopment of clavicles. Broad forehead | Medial portion of clavicles may be present; slim long bones | Autosomal recessive | Good |
| Osteogenesis imperfecta congenital | Deformed short limbs with multiple fractures and soft skull. Collagen studies may help in genetic counseling | Poor ossification of skull. Multiple fractures of other bones | Heterogeneous group probably with dominant and recessive types (Sillence & Rimoin 1978) | Poor |
| Hypophosphatasia (newborn type) | Soft skull (caput membranaceum) with short deformed limbs. Plasma calcium and urinary phosphoethanolamine raised | Caput membranaceum and poor ossification of whole skeleton | Autosomal recessive | Poor |
Osteochondrodystrophies manifested later in life:
| Name | Major clinical features | Radiological feature | Inheritance |
|---|---|---|---|
| Hypochondroplasia | Mild form of short-limbed dwarfism (adult height 117-148 cm) not usually apparent until three years of age. Face and skull normal, apart from slight bossing of forehead. | Rather short, widened long bones with slight flaring of metaphyses. Variable and may be mild. | Autosomal dominant but distinct from true achondroplasia |
| Dyschondrosterosis (Leri-Weil syndrome) | Mild mesomelic dwarfism with Madelung’s deformity of the wrist. Radius, ulna, tibia and fibula are short and wide. | Bowing of radius with hypoplastic distal end of ulna | Autosomal dominant with increased severity in females |
| Metaphyseal chondrodysplasia | There are many sub-groups in this category, all of which show mild short-limbed dwarfism, irregularities of metaphyses and normal epiphyses and spine | ||
| 1. Jansen type | Most severe of group-patients develop large joints and contractures. Mandibular hypoplasia. Severe shortening | All metaphyses severely involved, legs worse than arms | Autosomal ? dominant |
| 2. Schmid type | Most common form moderate short stature bow legs and waddling gait | Major bones affected worst – hands and feet often spared | Usually autosomal dominant |
| 3. McKusick type (cartilage-hair hypoplasia) | Moderate dwarfing. Hands loose jointed. Legs bowed. Hair light, sparse and find and breaks easily. Skin pigmentation decreased | Relatively long fibula. Metaphyseal lesions worst at knees | Autosomal recessive |
| 4. With malabsorption and Neutropenia (Schwachman) | Pancreatic exocrine deficiency. Cyclical neutropenia | Variable metaphyseal dysplasia | Autosomal recessive |
| 5. With thymo-lymphopenia | Lymphopenia agammaglobulinaemia and thymic hypoplasia. May be ectodermal abnormalities | Metaphyseal flaring. Abnormal pelvis-but normal hands and skull | Autosomal dominant |
| Spondylometaphyseal dysplasia (Kozlowski) | Short trunk dwarfism with kyphoscliosis (may be confused with Morquio’s disease). Growth retardation from 1-2 years. Adult height 130-150 cm. Waddling gait and stooped posture | Generalized metaphyseal irregularity especially affecting femoral neck, platyspondyly and abnormal pelvic bones | Autosomal dominant |
| Multiple epiphyseal dysplasia (Fairbank etc.) | Several disorders with mild / moderate short stature with short limbs and epiphyseal dysplasia. Adult height 138-166 cm. May lead to waddling gait and pain and stiffness of joints especially hips. May be misdiagnosed as Perthes’ disease | Symmetrical irregularity and poor development of epiphyseal ossification centers, especially those of legs | Usually autosomal dominant but recessive forms described |
| Hereditary arthro phothalmopathy | Severe progressive myopia from early childhood, leading to retinal detachment and blindness. Short stature is not marked | Similar to mild (Sticker) spondyleopiphyseal dysplasia | Autosomal dominant |
| Pseudoachondroplastic dysplasia | Rhizomelic short-limbed dwarfism, with normal trunk and skull which becomes apparent at 2-3 years. Adult height 91-138 cm. Waddling gait. May be lax ligaments. Precocious osteroarthritis of hips | Generalized involvement of epiphyses and metaphyses of long bones and platyspondyly | An heperogeneous group of disorders with dominant and recessive types |
| Spondyloepiphyseal dysplasia tarda | Mild form of short trunk dwarfism in males with premature osteoarthritis and epiphyseal dysplasia involving spine and hips. Growth failure evident from five to ten years. Hands, feet and head normal. Adult 131-157cms | X-rays normal in early childhood; later, abnormalities of spine, initially of the lumbar vertebrae in adolescence | X-linked |
| Acrodysplasias | A number of disorders with mild short stature and shortening of hand and feet bones; some associated with mental retardation (acrodysostosis) or odd facies and hair (trichorhinophalangeal syndrome) | - | Dominant and recessive forms |
Tool and Technology
1. Antenatal MRI
Dr Sona A Pungavkar, DNB, DMRD., Consultant, Dr Deepak Patkar MD
MRI Centre, Nanavati Hospital, Vile Parle, Mumbai
Magnetic resonance imaging (MRI) was first used in prenatal diagnosis in the early 1980’s. It became obvious that, MRI allowed for greater resolution of the fetus as compared to the commonly used ultrasound. MRI is the ideal choice because of lack of ionizing effect, multiplanar capability and inherent soft tissue contrast. Although seen as a promising technique, fetal MR studies were limited by long image acquisition times that necessitated sedation of the otherwise moving fetus. Technical advances of the early 1990’s produced fast MR techniques, better coils and gradients. This paved the way for meaningful imaging of a fetus without the need for sedation. Single-shot fast spin echo (ss FSE) sequences provide evaluation of the fetal organs, especially of the brain in a detailed fashion.
Aim: This study was performed
1. To establish the efficacy of antenatal MRI.
2. To ascertain if antenatal MRI could provide additional information compared to ultrasound
In a prospective study, we performed antenatal MRI in 60 abnormal pregnancies of which, 04 were multifetal pregnancies. The fetal gestational age ranged from 15 to 37 weeks. We highlight the cases of abnormal fetal spine and limbs. These are five in number.
Method:MRI was performed on a 1.5 T Signa, Echospeed machine (GE Medical Systems, Milwaukee, USA). A torso-phased array or body coil was used depending on the age of the scanned in the supine position. 2 patients in the third trimester were uncomfortable in the supine position and were scanned in the left lateral decubitus position. The entire gravid uterus was first scanned in three planes orthogonal through the fetal organ of interest. Each sequence was then used a scout for the subsequent sequence, depending on the indication and the target organ. ssFSE sequence was used. The scan time per sequence was ranging between 15 to 23 sec. Minimum slice thickness obtained was 2 mm and the maximum was 6mm. The sequence was repeated in cases where fatal motion caused artifacts. 3D reconstructions were also obtained in few patients.
Results:The MRI study was well tolerated by all patients and no patient experienced significant discomfort, so as to abandon the study. In all the patients, satisfactory images could be obtained in multiple planes. The anatomy was displayed and interpreted with respect to the fetal orientation. In all the cases, MRI provided as much information as the ultrasound. Additional information was obtained in 3 patients, while better delineation was provided in 2 patients. Of these, significant contribution to the prenatal counselling and pregnancy management was observed in all 5 cases. There were no contradictory findings between the two imaging modalities.
2. Biomechanical & Biophysiological Interpretitions Of The Cubitus Varus Deformity Following Supracondylar Fractures
(A cadaveric experimental study & follow up of the 412 cases of supracondylar fractures between 1990 & 2003)
Dr DC Srivastava MS, Dr SC Gaur MS
George Town Allahabad
We have conducted an experimental study on a right upper limb of a 15year old cadaver. We have denuded the muscles from the humerus, radius & ulna. We have preserved the elbow joint complex with their capsules & ligaments. We produced an artificial fracture at supracondylar level by transverse osteotomy. We passed a K wire through the medullary canal of the humerus & a K wire through the medullary canal of the ulna. The third K wire was passed in the distal fragment of the humerus parallel to the fracture line & perpendicular to the humeral K wire. We used the specially designed goneometre to measure the angles when the fracture site is subjected to the r~ different a type of angulation & rotations.
We are of the opinion that the cubitus varus deformity following supracondylar fractures are produced due to medial angulation or medial rotation or due to the combination of the both immediately after the fracture unites & we are capable of measuring the carrying angle when the full extension & full supination is possible following the physiotherapy. The change in the growth of the medial or lateral condylar epiphysis does not play an important role at that time because that time period is so short that the growth changes can not produce any significant impact.
The 412 cases attended our clinic between 1990 & 2003. The 390 cases were treated conservatively by close reduction followed by POP cast & 22 cases were treated by open reduction & fixation with K wire. The 320 cases showed no change in the carrying angle but 71 cases showed cubitus varus deformity ranging from 1 to 11 degree with an average of 5.4 o immediately after the treatment with return of the full supination & full extension.
The 200 cases with normal carrying angle, 21 cases with cubitus varus & 6 cases with the cubitus valgus deformity were lost in the follow up. But 120 cases with normal carrying angle, 50 cases with cubitus varus deformity & 15 cases with cubitus valgus deformity were followed from 6 months to 13 years with an average of 5.7 years.
In the 120 cases with normal carrying angle showed changes in the angle with development of cubitus Vanls deformity in 13 cases ranging from 1 to 13 degree with an average of 4.4 degree & cubitus valus deformity in 2 cases with 50 in one case & 80 in second case. In the 50 cases with cubitus varus deformity, 40 showed no change but 10 cases showed increase in the angle ranging from 3 to 11 degree with an average of 4.8 degree. In 15 cases with the cubitus valgus deformity 11 showed no change but 4 cases showed in increase by 2 to 8 degrees.
The follow up findings indicates the growth variation in the medial or lateral epiphysis is also an important cause for the production of the change in the carrying angle & it plays it role only over a long period of time in the later phase of the growth after the treatment but no immediately during the phase of treatment.
3. Clinico Radiological Evaluation Of Perthes Disease – Is Surgery Needed In All Cases?
Dr. Harsimran MR, Prof. SS gill, Dr. MS Dhillon, Dr (Mrs.) Katariya
Deptt. Of Orthopaedics & Radio-diagnosis, PGIMER Chandigarh
30 cases of Perthes were studied to compare the ultimate range of movement and sphericity of the femoral head in patients managed conservatively and those undergoing surgery. The mean age of the patients was 6.34 years, male to female ratio, 10.6: 1 and 70% belonged to low socio economic group. 21 cases had Rt. Hip involvement, one bilateral and 8 cases had Lt. Hip affected. The diagnosis was made by classical clinical presentation and radiological features on plain X-rays (MRI & Bone scan being done in the doubtful cases). Out of 24 patients whose aged was less than 9 years, 8 had Caterall stage 1 & 11 and 16 had staged III & IV disease. 6 patients had disease onset after 9 years of age and all had stage III & IV disease. All stage I & II patients underwent conservative treatment consisting of traction, analgesics and calipers. Subtrochanteric derotation varus osteotomy was done in six patients with stage III & IV disease. All these patients were less than 9 years of age. Rest of the patients of stage III and IV disease received conservative treatment. The results were assessed at two year; from one of symptoms. Itangc of movement of hip in flexion, abduction and internal rotation was measured with a goniometer. The sphericity of the femoral head was measured with a Mose template using X-rays in AP and Frog lateral view. We did not find any statistically significant difference in the result in patient of stage III/IV Caterall, treated conservatively or by surgery. All patients with age >9 yrs at presentation had poor ultimate outcome.
4. Efficacy Of Botulinum Toxin – A In Cerebral Palsy
Dr Harsharan Singh Oberio MS, Dr Raju Shamla MSPT
Basant Memorial Trust, Oberio Hospital, Jalandhar, Punjab
The use of Botulinum toxin type A has gained widespread acceptance in clinical management of focal muscle spasticity seen in patients with Cerebral Palsy, Stroke and Traumatic Brain Injury. Purpose of study was to register the effects of BTX-A in reducing the spasticity and improvement in overall motor function.
Material and Method:23 children (average age 5 years) were given BTX-A injections (6 to 8 units/Kg.). Children were assessed before and after 3 months of injection for spasticity level, more function, range of motion and gait by MAS, GMFM, Goniometry and Observational Gait analysis respectively. Statistical analysis done using paired t test. Follow up was done at 6 months.
Results:78 percent children showed significant improvement (t at P<.001) in their spasticity level, motor function and range. On follow up only those who continued therapy, maintained their functional level.
Conclusion:BTX-A proved both safe and effective in management of focal muscle spasticity in C.P. However to maintain functional level continuing regular physiotherapy and parental support are very important.
Key-words:Spasticity, BTX-A, C.P., neuromuscular block
5. Management Of Tibfp: Ial Lenthening Using Ilizarov Apparatus And Botox To Prevent Equinus Contracture
Dr Sandip Vyas, MS (Orth.); D.N.B. (Orth.); Ilizarov Fellow (USA)
Purnima Hospital, Road No. 8, Daulatnagar, Borivli (E), Mumbai 400 066.
Seven patients underwent Tibial Lengthening with Ilizarov Apparatus without a Foot-frame. All patients were given Botox Injection (Sub Type 4). Two to Four units / kg. of Botox per muscle Belly of Gastrocnemius was used, and Ilizarov Apparatus applied.
Results:Mean Lengthening achieved was 4.5cms. Patients were on the regular Physiotherapy Protocol Post-Operatively. After frame removal, there was no equinus contracture in any patient. All patients underwent lengthening without significant pain and were walking comfortably without Foot-Frame.
Discussions & Conclusions:Botulinum Toxin Binds to Motor nerve terminals and blocks release of Acetylcholine. The action lasts for 4-6 months with reversibility of action due to sprouting of nerve terminals. This feature helps us to complete Lengthening with a Paralysed Gastrocnemius and prevention of Equinus contracture in spite of no Foot-Frame, without significant pain.
6. Non Factor Transfusion Management Of Hemophilic Synovitis Knee In Children
Dr SK Saraf, Dr OP Singh
Department of Orthopaedics, Institute of Medical Sciences
Banaras Hindu University, Varanasi, India
Complications of musculo skeletal bleed like synovitis usually present late. The repeated factor transfusions recommended, as gold standard for the prophylactic as well as for the management is not possible in developing countries like India due to shortage and high cost of factor transfusion. Due to these constrains, we used Pulse Ultra Sound Therapy and muscle stimulation along with exercises to manage our patients of Hemophilic synovitis of the knee to observe if it can be used as an alternative therapy.
Material & Method:Forty patients with 52 synovitis of knee selected at random and followed for minimum six months were considered as subject for the present study. Synovitis was classified as per Cavilgia (1997) classification. A total of 16-20 sittings of low frequency pulse ultrasound of six minutes duration five days a week were given. The results were assessed by observing the changes in the swelling, range of movement in the joint, frequency of joint bleed during the observation period and joint tenderness and classified as Good, Fair and Poor.
Results:The age of patients ranged from 5 – 15 yrs. Six knee belonged to Grade I, 24 to Grade II and 22 were classified as Grade III. In grade I, there was significant improvement in swelling and range of movements with decrease in pain and frequency of bleeds. In grade II also there was improvement in swelling, pain and range of movements. In grade II also there was improvement in range of movements, but no difference was observed in swelling and frequency of bleed. Overall results were assessed as Good in 16, fair in 22 and poor in 14.
Discussions & Conclusions:Pulse Ultrasound acting by its fibrinolytic effect and by enhancing the rate of absorption of hematoma helps in early recovery in synovitis of the knee. The results were better when the therapy was started earlier in the phase of synovitis. In long standing cases without arthropathy, the results were still encouraging. In developing countries, where patients present late and factor transfusion not always possible, PUSA with muscle stimulation can give the comparative results.
7. Partial Transfer Of Hamstrings For Crouch Gait In Cerebral Palsy
Dr Kunjabasi Wanhjam
HOD, PMR, RIMS, Imphal, Manipur
Crouch gait or posture is one of the most resistant conditions to treat in I cerebral palsy with spastic diplegia. Twenty nine such patients (19 males, 10 females); aged between 3 to 16 years (mean 8.9 years) were treated at the Department of Physical Medicine & Rehabilitation, Regional Institute of Medical Sciences, Imphal from Jan 1992 to December 2001 by partial transfer of distal hamstrings to correct croutch gait. Some tendinous and biceps by partial transfer of distal hamstrings to correct croutch gait. Some tendinous and biceps femoris tendons were transferred to lower femoral condyles by fixing to tendinous origins of corresponding gastrochemi. Semi-membranosus tendon was not transferred; but lengthened and it was left to serve as knee flexor. Results were assessed at 6 weeks, 3 months, 12 months after operation based on reduction of popliteal angle, increase of hip extensor power, improvement in balance and gait. Accordingly, 6 cases were graded as excellent; 16 as good; 2 as fair and there was no patient in poor grade. Genu-recurvatum occurred in 2 cases. Patients were followed up for a period ranging from 1 to 10 years (mean 5.5 years). This method of partial transfer of distal hamstrings is effective in relieving crouch gait, in spastic diplegic cerebral palsy.
8. Predicting Which Wlaking Aid Cerebral Palsied Child Will Need
Dr Dhiren Ganjwala
Ganjwala Orthopaedic Hospital, Ahmedabad, India
Spasticity and deficient equilibrium are two major problems of cerebral palsy child which case difficulty in ambulation. To overcome deficient balance child need some sort of supporting device. The aim of this study is to establish correlation with deficiency in equilibrium and supporting aid child needs.
Material & Method:40 children with cerebral palsy were enrolled in the study. All the children were diplegic and ambulatory. 26 children had undergone some orthopedic surgery in the past. Children were tested for their capacity to maintain equilibrium in anterior, posterior and right and left direction. Their preferred device for support was asked. When they were using more than once device, they were asked to walk with each device and their energy consumption was measured by change in the heart rate and time taken to cover 30 feet distance. The device which gives lowest physiological cost index was considered as preferred device. From equilibrium deficiency, children were divided into five groups. Group A has adequate balance in all 4 directions. Group B has deficiency in one direction or has good balance in 3 directions and Group E has deficiency in all 4 directions. Children were either walking with the help of walker )4 point support) with two crutches, single crutch / stick or independently.
Results:| 4 point walker | 2 crutches | Crutch/stick | Independent | |
| Good in 4 directions | 9 | |||
| Good in 3 directions | 6 | |||
| Good in 2 directions | 4 | 5 | ||
| Good in 1 directions | 12 | |||
| Good in 0 directions | 4 |
Independent walker has good balance in 3 or 4 directions. While those who depend on 4 point walker have poor balance in all 4 directions or in 3 directions. The results indicate that simple test of checking equilibrium guides clinicians to select the best supporting aid for ambulatory cerebral palsied child.
9. Rectus Femoris Transfer For Childrenwith Cerebral Palsy – A Lng Term Outcome
Dr Aik Saw, FRCS (Edin), Dr Peter A Smith, MD, Dr Yuddasert Sirirungruan, MD, Dr Chen Shande, Ph.D., Dr Sahar Hassani, MS, Dr Gerald Harris, Ph. D., Dr Ken N Kuo, MD
Introduction:The purpose of this study was to evaluate the long term results of Rectus Femoris Transfer (RFT) in cerebral palsy children with stiff knee gait by gait analysis and functional ambulatory assessment.
Materials and Methods:Thirty-eight affected limbs in 24 children were evaluated by comparing preoperative and one year postoperative gait analysis. Also included were 26 limbs in 18 patients that were evaluated during a second gait analysis after an average of 4.6 years following surgery. Functional ambulatory status evaluation was based on level of ambulation as defined by Hoffer, 8 requirement of walking support and usage of ankle brace. Improvement or deterioration was documented at one year after surgery and at final clinical review at a mean of 5.6 years.
Results:There was statistically significant improvements of 9.8 degrees in maximum swing phase knee flexion and 7.0 degrees in total range of knee motion at one year as measured by gait analysis, with a slight loss of knee extension in stance (3.70, p=.03). At long term gait analysis, the improvement in the swing phase knee flexion was maintained, but improvement in total range of knee motion was decreased due to further loss of knee extension (70, p=OOOI). There were no significant changes in temporal parameters either at one year or at the last gait analysis. Eight children showed improvement in functional status of their ambulation while five (not four) deteriorated at one year after surgery. At the final follow up, ten children showed clinical improvement while three deteriorated in their ambulatory status after surgery.
Conclusions:Improvement in swing phase knee flexion and foot clearance after RFT was associated with loss of knee extension at long term follow-up. Hamstring lengthening in patients who develop excessive stance phase knee flexion, as well as careful attention to rotational abnormalities of the femur and tibia, and foot valgum may be necessary. There were more functional improvements than deteriorations in ambulatory status following RFT. Cerebral palsy children may require a longer period to recover from surgery and evaluation at times farther out than 12 months with gait analysis may be required.
10. Study Of Post Polio Residual Paralysis Around Ankle And Foot
Dr Preshit Gaddam, Dr OP Sharma, MS, Dr KR Patond, Professor & HOD Sewagram,
Wardha 442102 Maharashtra, India
Modern Orthopaedics deals with the study of the form and the function of the musculoskeletal system. Poliomyelitis which is known to be an oldest disease of mankind has been almost wiped off from the developed countries. However in developing countries poliomyelitis still continues to be one of the health problems of pediatric age group’.
Material and Methods:62 patients suffering from post polio residual paralysis around the ankle and foot with lower limb involvement were examined and managed in the department of Orthopaedics, MGIMS, Sewagram. Muscle imbalance and deformities around the ankle and foot constituted the study. Thorough history clinical and neurological examination was carried out. Plan for management was laid down. All the surgeries were done under G.A., under tourniquet. Some patients with severe deformity were given traction before definitive surgical procedures.
Results:Out of 62 patients, 53 (85.5%) were inpatients and 9 patients were treated on OPD basis. There were 24 males and 21 females. Majority of patients seen in were 7 to 9 years of age group with female predominance. Right lower involvement was common. Bilateral involvement was equally common (27 patients, 43.5%). Equinus deformity with its variant was the common deformity. Muscle wasting and shortening of lower limb was a constant feature. Tibialis anterior and posterior were the commonest muscles involved. 36 patients offering 38 feet (2 bilateral cases) were operated upon. 35 tendon transfers done Total 87 orthotic appliances were prescribed and supplied to the patient.
Discussion:Study and its results were comparable with other series in India. The paper will highlight the same.
Conclusion:Prevention is better than cure, stands very much in poliomyelitis. However, if a person has been affected by poliomyelitis, all the possible measures should be undertaken in preventing the severe deformities and definite treatment should be instituted at the earliest to provide reasonably useful limb.
Poster Presentation : Congenital / Developement
1. Accessory Soleus Muscle – Presenting With Rigid Club Foot Deformity, A Report In 3 Feet
Dr. P. N. Gupta, Dr. Raj Bahadur
Department of Orthopedics, Govt. Medical College & Hospital, Chandigarh
Clubfoot is amongst the commonest of congenital skeletal anomalies. It usually presents as isolated deformity; the incidence of associated anomalies is about 6%. We came across 3 such clubfeet in 2 children with associated accessory soleus muscle. The purpose of presenting this study is to know the contribution of this muscle to the deformity and to propose treatment method for dealing with such abnormality.
Case Report: Case 1:A one year male child presented with right sided rigid clubfoot and was planned for posteromedial release. During dissection, and accessory soleus muscle inserting on to posteromedial aspect of calcaneum was revealed (Fig.). To assess the contribution of the equinus persisted. Full correction was achieved only after tenotomizing the insertion of this muscle. At 1 year follow up; the patient is walking with a plantigrade foot.
Case 2:A one year male child presented with bilateral rigid clubfeet. Bilateral soft tissue release was done using Cincinnati incision. Accessory soleus was present on both sides and in this patient also, full correction of deformity was achieved only after tenotomizing the insertion of this muscle.
Discussion:An accessory muscle forms due to splitting of a muscle anlage during fetal life. Soleus muscle fuses with the Gastrocnemius at the middle and lower third junction of leg to form the tendoachilles; accessory soleus tendon inserts separate from tendoachilles on the calcaneum. The most common presentation of accessory soleus is by a swelling at the posteromedial aspect of the ankle in early adulthood; associated with clubfoot is less common. The accessory soleus muscle contributes to a rigid deformity as was observed during surgery in both patients. When present, surgical division of this muscle along with posteromedial soft tissue release achieves full correction of the deformity.
Conclusion:Accessory soleus muscle when present in clubfoot contributes to rigid deformity; though may not be sole cause of deformity. Full correction requires surgical division of the muscle in combination with a soft tissue release.
2. Assessment Of Clubfoot Deformity Using Dimeglo’s And Pirani’s Scoring System
Dr. Hailendra Telang, Dr. Taral Nagda, Dr. Vikas Trivedi
Department of Orthopaedics KEM Hospital Parel Mumbai
We conducted a study involving 22 idiopathic clubfeet in 15 pts over a period of 6 months, comparing DIMEGLO’S & PIRANI’S scoring systems for assessment of clubfoot deformity, while treating the children with the PONSETI’S method of clubfoot correction. The goal of study was to apply both these studies to practical use and to determine inter & intraobserver reliability of these systems and to study the co-relation between the different parameters of both these systems.
Materials & Methods:Two designated observers evaluated 22 feet over a period of 6 months, a total of 144 examinations.
Results:The children ranged in age from 1 to 6 months with mean age of 3.3. Both the scoring systems demonstrated excellent inter-observer reliability with correlation coefficients of 0.9915 (Pirani) & 0.9638 (Dimeglio). The 95% confidence intervals were within 2.3 points (Pirani) and 4 points (Dimeglio). Both the scoring system demonstrated excellent intra-observer reliability with the first examinee having p-values of 0.9658 (Pirani) & 0.9399 (Dimeglio). The three parameters of the hindfoot score in the Pirani systems went hand in hand throughout the course of the treatment out of 22 feet scored, 18 feet(82%) had the scan scoring of all 3 hindfoot parameters without any change.
Conclusions:Both Dimeglio’s and Pirani’s classification systems have a good inter observer and intraobserver reliability. The three parameters in the Pirani’s hind foot score did not show any variation, thus the need to merge them into one single parameter to represent the hindfoot score and further simplify this scoring system should be considered.
3. Congenital Bilateral Pseudoarthrosis Of Hemerus
Dr Sanjay Yadav, Dr Shailendra Telang, Dr Taral Nagda
Seth GS Medical College & KEM Hospital, Parel, Mumbai
Congenital pseudarthrosis is a known common entity especially of tibia, studied in detail in the literature. These have been associated with a variety of multisystemic conditions like Neurofibromatosis. The age of presentation and the outcome of these states are well studied in Indian and western literature. We present a case of congenital Pseudarthrosis of humerus in a 3 year old male child who presented with bilateral deformities of the arm since birth. There were no sings of presented with bilateral deformities of the arm since birth. There were no signs of neurofibromatosis in the family or in the patient. Of his five siblings one sister was diagnosed as Beals congenital arachnodactyly. Other siblings were normal. Routine X-rays showed middle third and lower third pseudarthrosis in both arms and elbow was free and mobile with no stiffness whatsoever. Blood parameters were normal. Detailed paediatric research laboratory assessment was done to rule out any systemic involvement of subset of any multisystemic condition. These turned out to be negative. MRI was done to assess the status of the joint. It revealed synovial type of joint with presence of fluid in between.
Surgical intervention was done on one side through anterolateral approach and stabilized with plate and fibula on lay graft. Intra-operative there was true synovial lining the pseudarthrosis with pseudo capsule and true synovial fluid. The sample was sent for histopathological analysis including electron microscopy to find any hamartomatous tissue of neurofibromatosis. The report was negative with indication of true synovial joint. Immediate post-operative Shoulder spica was given and mainted for a period of 6 weeks. At six weeks there was good radiological and clinical union. The other side was operated at 2 ½ months after first surgery with predictable outcome. Congenital pseudarthrosis of humerus is not described in literature. Analogy is drawn to the post-infective or post-trauma pseudoarthrosis, both which were absent in this case. Out detailed investigations to rule out any underlying cause or pathology yielded no result, suggesting of its idiopathic nature. Our management produced predictable result with good outcome.
4. Cross-Leg Sitting Test In Tarsal Coalition
Dr Atul Bhaskar
Guru Nanak Hospital, Gandhinagar,
Bandra (East), Mumbai 52
We describe a new finding that can alert one to the presence of a tarsal coalition Cross-leg sitting test requires the subject to sit with his hips and knee flexed and feet inverted. An inability to sit in this position and, the knee of the affected leg at a higher level for comfort may be due to a presence of a stiff hindfoot.
Introduction:Tarsal coalition is an uncommon condition seen in children and adolescents. Symptoms appear when there is loss of motion in the hindfoot due to ossification of the coalition. Some children may present with vague aching pains around the hindfoot for years and there may be history of recurrent ankle sprains. The classic findings of heel valgus, peroneal spasm and abducted forefoot clinches the diagnosis, but these characteristics take years to develop. We describe a simple clinical test that may alert one to the presence of a tarsal coalition before the above changes develop. Thus early management may help control the symptoms and prevent delay in surgical treatment.
Method:The test comprises sitting cross-legged on a firm flat surface. Normal cross leg sitting requires good hip and knee motion and also a flexible hindfoot to invert the heels. In normal cross-leg sitting the knees are at the same with each other. As one attempts to sit cross-legged with a stiff hindfoot, the inability to invert the heel in the presence of normal hip and knee motion causes the knee of the affected leg to assume a higher level. This asymmetry in the sitting posture can provide a clue to restriction of hindfoot motion. Further clinical and radiological examination in a child can then be pursued to establish the diagnosis. In bilateral tarsal conditions, both the knees may be at a higher level and the asymmetry in the knee position may reflect the degree of hindfoot motion. We performed this test on six children complaining of hind foot pain. Four children demonstrated positive cross-leg sitting test and the subsequent radiograph confirmed a tarsal coalition – three had talocalcaneal and one had calcaneonavicular coalition. In the other two children the radiographs were normal.
Discussion:Most tarsal coalitions are aymptomatic and they often remain so in adulthood. Children with alcaneonavicular coalitions become symptomatic earlier as compared to those with talocalcaneal coalition. The usual age for children to be symptomatic is between 8-12 years in the former and 12-16 year in the latter. The cross-leg sitting test should be performed in any child complaining of foot pain provided there is normal hip and knee motion. Imaging studies for evaluation of a patient suspected of having a coalition includes radiographs of the entire foot and oblique views of the subtalar joint. A CAT scan is usually required to confirm the diagnosis and map the area of the coalition. Early diagnosis and treatment of the coalition, before secondary changes occur in the hindfoot can lead to permanent resolution of symptoms and relief of pain.
5. Management Of Ctev By Ponseti Method
Dr B Leela Prasa, Dr M Murali Mohan, Dr KS Praveen Kumar
Background:Idiopathic CTEV is one of the most common congenital deformities. Traditional methods of conservative management have yielded only fair results with considerable incidence of recurrence and surgery. Ponseti started his method of serial casting for CTEV in early 60’s and has reported 88% success rate in long term follow-up(Ponseti, 1980)
Aim:To assess the effectiveness of Ponseti method of serial casting for correction of CTEV.
Materials and Methods:20 patients with 34 feet, in the age group of 0 to 4 months were treated with serial casting during the period January 2003 to October 2003.
Results:We assessed our results as per the CLINICAL CLUB FOOT SCORE devised by Royal Columbia Hospital, University of British Columbia. Our success rate was 91%.
Conclusion:Ponseti method of serial casting is an easy effective and economical method for the management of CTEV. Even though our follow-up period is short ((<)one year), our success rate (91%) is definitely encouraging.
6. Ponseti’s Technique – A Noble Approach To Club Foot
Dr. R. A. Agrawal, (MS Ortho), Dr. Anuj Kr. Jain (D Ortho.)
Agarwal Orthopaedic Hospital, Jubilee Road, Gorakhpur, UP, India
Phone – 0551 – 233102, Email – agrawalram@hotmail.com
All Idiopathic club feet are treated with preliminary serial casting. However, 70-95 percent cases need Postero Medial Research (PMR) surgery, which leads to long-term stiffness and weakness. Ponseti stands for surgery only in 11 percent of patients.
Material and Method:25 young children (33 feet) were treated by this method. Serial casting begins within first six months of life. Abduction applied to metatarsals, counter pressure on neck of talus not calcaneus, never pronate the foot. Weekly casting for 4 to 7 weeks, Percutaneous Achilles Tenotomy under local anesthesia in 90% cases, casting for three weeks followed by foot abduction arthrosis 23 hours a day for three months and night time for three years. Only 10% needs anterior tibialis tendon transfer at the age of 2 ½ to 4 years.
Result:| PMR surgery required | Average duration of casting | Final Dorsiflexion | Final Plantar flexion | |
| Ponseti Group | 1/33 (3%) | 2 months | 32° (10-45°) | 50° (25-70°) |
| Control Group | 31/33 (94%) | 3 months | 80 (5-20°) | 29° (10 –40°) |
- Our study shows successful results in 25 cases.
- Simple
- Highly effective
- Less expensive (less need for hospitalization)
- Eliminates need for PMR in vast majority of patients)
- Leads to stronger, more flexible feet and better long-term outcomes
Based on our success, we no longer think that PMR is required for most cases of idiopathic clubfoot. Longer follow-up will determine whether we can continue to match Ponseti’s reported outcomes.
7. Role Of Intraoperative Radiography In The Assessment Of Resmual Deformity In CTEV
Dr. Karanu Karan, Senthil Nathan S, Prof S.S. Gill
PGIMER, Chandigarh
In this study, 22 patients were subjected to intraoperative stress radiography using Simon’s standardized technique. Radiographic measurements were made for each of the deformities in hindfoot, midfoot and forefoot. Postoperatively, the foot was assessed using Demiglio score for residual deformity by a blinded experienced observer. The sensitivity, specificity, false positive and false negative values of each of the intraoperative radiological measurement were made. It was evident from our study that some of the radiological parameters like Beatson index for varus, talo-first metatarsal angle (AP) and calcaneofith metatarsal angle (AP) for forforehood adduction and calcaneo-fifth metatarsal angle (lateral) for cavus are highly sensitive and can be used routinely intraoperatively. However other radiological measurements for equinus, talonavicular dislocation should be used with caution.
8. Short Term Results Of Ponseti Method For Clubfoot
Dr Dhiren Ganjwala
Ganjwala Orthopedic Hospital, Ahmedabad, India
Clubfoot is very common congenital foot deformity. Various treatment methods like gentle manipulation, strapping, brace, repeated corrective cast and surgery have been described for this deformity. The aim of this paper is to study results of Ponseti method of plaster treatment.
Material & Method:34 idiopathic clubfoot in 22 patients under the age of 6 months were treated with Ponseti method. Average age at the time of starting the treatment was 1.2 months (ranging from 1 day to 5 months). Three feet in three patients had taken plaster treatment elsewhere without achieving full correction. Severity of clubfoot was assessed by Pirani severity scoring before starting treatment. All patients were given plaster as per the standard technique of correction recommended by Ponseti. Average number of plaster were 4.3 (ranging from 3 to 7).
All patients completed the treatment. Full correction was achieved in all but one patient. In a child in whom full correction was not achieved, treatment was started at all age of 5 months and was treated by 6 plasters before staring Ponseti technique. Only cavus did not correct completely while other components of deformity got corrected. Not a single child required surgery other than percutaneous tenotomy of tendo Achilles. 4 feet in four patients showed early signs of recurrence and were managed with one plaster in a position of more than 50 degrees of forefoot abduction for 3 weeks. All feet were evaluated at average of 15 months after treatment (range from 6 months to 24 months).
Results:Results were evaluated clinically and parents satisfaction at the time of latest follow up. On clinical examination, degree of correction (by Pirani severity scoring) and range of motion were tested. Parents were asked whether they are happy with the correction or not and whether they will suggest this treatment to some one. 33 feet out of 34 had complete correction of all component of clubfoot. Pirani severity score dropped from 4.9 before treatment to less that 0.5 at the time of latest follow up. All parents were happy with the treatment and said that they will like to recommend this treatment to someone with clubfoot.
Conclusions:The results achieved in this study suggest that Ponseti treatment produces satisfactory correction in 97% of idiopathic clubfeet.
9. Spectrum Of Congenital Orthopaedic Anomalies In The Department Of Orthopaedics, M.G. I.M.S.
Dr Kiran Kumar Mallam, PG, Dr Balvinder Rana, MS, Dr KR Patond, Prof. & HOD
Department of Orthopaedics, Mahatma Gandhi Institute of Medical Sciences
Sewagram, Wardha 442102 Maharashtra, India
The musculoskeletal system is the one most prone to congenital anomalies, yet the full spectrum & anatomic variability of its anomalies is not well appreciated. Indeed the complicity of its growth and embryology make it unusually vulnerable to anatomic variability.
Material & Method:This study was conducted in the Department of Orthopaedics, Mahatma Gandhi Institute of Medical Sciences. All patient reporting a out patient to the Department of Orthopaedics with congenital orthopaedic anomalies were included in the study. The details were described in a pre-designed proforma and thorough examination was done to exclude other congenital anomalies.
Observation & Results:Among the 172 patients, 190 anomalies were observed (multiple anomalies in 18 patients). These 172 patients were among total 18006 new patients who reported to the department accounting for 0.98% of cases 31 different types of anomalies were observed. CTEV was common, i.e. 49.4% of cases. Rare anomalies in form of hemimelia, foot on knee were observed.
Discussion:The magnitude of such anomalies may not be very great when considered in comparison to other affections of the musculoskeletal system. Still these are important. The study results are comparable to other studies but a single study insufficient to answer all the questions and more similar studies are required to substantiate any of the above statement.
Conclusion:To have been born and grew up with anomalies is very frustrating for the child and become a stigma for the adult patient. Once the exact spectrum and burden of these anomalies well documented, efforts can be directed to their effective prevention and treatment.
Poster Presentation : Infection & Arthropathy
1. Body Mass Index In Infants: Predictor For Bow Legs?
Dr Atul Bhaskar –Paediatric Orthopaedic Surgeon
Children Orthopaedic Centre, Guru Nanak Hospital, Gandhinagar, Bandra E, Mumbai - 400 054
Minimal to moderate bowlegs is normal in infancy. These children present at the walking age with wide-spaced gait, toeing-in and occasionally repeated falls. An orthopaedics consultation is usually sought to allay parental anxiety. We looked at 10 infants before walking age and calculated their Body Mass Index (height / weight2) A low BMI can predict the excessive physiological varus (>16 degrees). Dietary modification can be helpful and fortunately all of these deformities correct spontaneously.
Patients and Methods:20 patients before the walking age were evaluated. In 10 infants (Group A) the weight was more than 90th percentile at the time of birth and in the other 10 patients (control group) the weight was between 50th and 70th centile. In all children the height (length) and weight were recorded at 9 months and 12 months. BMI was calculated for both the groups at 9 months and one year. In both groups the mean tibio-femoral angles were measured clinically and radiologically.
Results:The mean BMI in Group A at one year was 0.35 and in the control group was 0.74 in both groups. In Group A the mean tibio-femoral angle at 18 months was 20 degrees. (14 degrees to 24 degrees) and in Group B it was 12 degrees (8 – 16 degrees). Two patients in Group A had varus of 14 degrees and one patient in group B had tibio-femoral angle of 16 degrees. Six of the Group A children at 3.5 years had complete resolution of excessive varus while the remaining four are still under follow up. Radiographs in these patients were unremarkable and they also had a normal calcium profile.
Discussion:Children with high birth weight continue to maintain their weight up to infancy and this may reflect as a low BMI. The mean birth weights at one year for Group A was 13.5 kg and for Group B was 9.8kgs. The two children in Group A who did not exhibit excessive varus had BMI of 0.44 and 0.48 respectively. Thus only weight may not predict the development of bow legs.
Conclusions:Low BMI at one year can predict excessive bow legs (> 16 degrees) and treatment can be focused on dietary modifications and reassurance then advising braces or splints. Further studies are required to elucidate the role of BMI in the development of angular deformities in children.
Poster Presentation : Spine
1. Histology Study Of Nerve Endings In Flava Ligament In Patients With Discopathy
Dr Raisi, Sh. Dr Raj Behadur.Z. Ph.D. Mardani, M.PhD. MoinH. MD
Isfahan University of medical sciences and Health Services
Histology study of nerve endings in flava ligament in patients with discopathy
Flava ligament normally has neural ends so it has sensory role and help to protect vertebral column against different injuries. The aim in this study is to detect the neural ends in flava ligaments in patients with discopathy.
Method:The samples were taken from flava ligaments of the patients with discopathy during surgery. One hundred samples were considered. Five Hundred sections were obtained and stained with H & E method and were studies with light microscope.
Results:Nerve corpuscles were found in none of the sections of the patients.
Discussion:It seems that flava ligaments in patients has a loss in the nerve ends that leads to a decrease in proprioceptive information to control nervous system and may injure tissues like cartilage, osseous and fascia.
Keywords:Discopathy, Nerve ends, Flava Ligament.
Poster Presentation : Tool and Technology
1. Correction Of Flexion Deformity Knee In Polio By Ilizarov Technique
Dr RA Agrawal MS
Agrawal Orthopaedic Hospital, Jubilee Road, Gorakhpur, UP, India
Phone – 0551 – 2333102, Email – agrawalram@hotmail.com
Joint contractures are common sequelae in Polio. In Polio flexion contracture of knee is commonest problem. If contracture is mild, patient will walk with limp. If moderate with hand knee gait, if severe walk with stick provided opposite limb power is near normal. Many surgical procedures have been performed since long like hamstrings tenotomy followed by manipulation, release of tensor fascia latae as described by Yount’s posterior capsulotomy fixed with the plaster.
Principle of correction of deformity is to bring the center of gravity of tarso to G.R.V. (Ground reaction vector) that is perpendicular line drawn from T10 it should be within the foot area. Thus the line between G.R.V. and C.G. should be straight one. Between 1994 and 2003, 14 cases with knee flexion contracture were treated by supracondylar extension osteotomy of femur and lengthening fixed with Ilizarov ring fixator.
If there is associated, hip flexion deformity that is tested by moving the patient on both the knees. If they are not able to walk properly in kneel gait, it means hip is unstable and hip deformity should be corrected first. It foot and ankle are also associated with knee deformity it should be corrected in second stage. The femoral osteotomy is done after fixing the femur with two Ilizarov ring and one arch then percutaneous supracondylar extension osteotomy is done closed to condyles and desired angle deformity is corrected. Lengthening is started after two to three weeks.
The advantages of this technique are that correction of deformity & lengthening can be done simultaneously. As the patient is mobile through out the period any redisual deformity can be treated along with it.
2. Osteotomy Treatment For Spastic Limb Deformities
Dr RA Agrawal, MS (Ortho.)
Agrawal Orthopaedic Hospital, Jubilee Road, Buxipur, Gorakhpyr – 273 001, UP (India)
Ph.No. – 0091-551 – 2333102, Email: Agrawalram@hotmail.com
The incidence of Cerebral Palsy is increasing globally. No cerebral palsy child has a spasm or contracture before birth or in neonatal period and all these clinical phenomenon develop with the growth of the child. Of all the clinical manifestations of cerebral palsy spasticity remains most dominant and if left unabated it gradually leaves various contractures and further deformities. The principles of management of cerebral palsy can be considered as:
- Wining over spasm: By pharmacological preparations and exercises.
- Surgery: In Cerebral Palsy surgery is mainly performed on the followings:
- Peripheral nerves
- Tendons – Tenatomy, tendon transfers
- Bony procedures – Osteotomy plays a bigger role in correcting the fixed deformities. Various stabilization operative procedures on the joints definitely correct the deformities and improve stability.
- Improving the power of muscles by proper scheduled physiotherapy.
The present work concerns mainly on the role of osteotomy in correcting the deformities in lower limb, mainly flexion, abduction, and internal rotation at hip; flexion deformity at knee and sever equinus, varus, cavus, abduction/adduction deformities at ankle foot. In the present work osteotomized fragments are controlled by Ilizarov Ring Fixator. The observation is based on 8 osteotomy in intertrochantric, 10 in region of femur, 1 at upper end of tibia and 10 in forearm (to correct pronation contracture). Due to some overlap at the osteotomy site little shortening is expected, which did not effect the ultimate results since problems are bilateral. Over all results have been quite encouraging.
3. Painful Hip In Children
Dr Anshuman Dutta
JNMC, AMU, Aligarh
- Prospective study conducted on 56 children below age group of 15 years.
- Non traumatic hip direction producing grain considered
- Decease encountered. TSH, Septic Arthritic, SCFE, Perthes Disease, DDH, JRA, T.B., etc.
- Managed conservatively or surgically according to A
- Tools used in writing has diagnosis:
- Clinical
- Radiological
- Laboratory
4. Torticollis – Sternomastoid Release Or Lengthening?
Dr S Sengupta, Dr Saw Aik
University Hospital, Kuala Lumpur
Though conservative and expectant management for muscular torticollis often succeeds, there is 10% to 20% failure rate. If untreated an ugly deformity is produced with gross limitation of neck movements and facial asymmetry. Early surgical release of stemomastoid muscle is carried out to get neck movements back to normal and avoid permanent facial deformity. However, this may result in an ugly scar, lateral fibrous bands and conspicuous loss of the STM column. For many years authors have instead, devised a way to elongate the tendon which gives a better cosmetic result. Deformity can be fully corrected with retention of STM column and an inconspicuous scar. Through a 3cm skinfold incision just proximal to sterno-clavicular joint, both heads of STM are exposed. The tendinous sternal head is cut proximally at the musculo-tendinous junction and the fleshy clavicular head is detached from its insertion on clavicle. The two ends are sutured to each other. Halter’s neck traction is applied for a few days, followed by vigorous stretching exercises.
49 patients between one and a half years to 20 years, operated in our institution were followed up for a median period of 4.5 years. Excellent to good results were achieved in 39 patients. In 5 the two ends could not be sutured to avoid too much tension and in others restoration of neck movements were not adequate.
Poster Presentation : Trauma
1. BIL SCFE – RT. – LT.
Dr Anshuman Dutta
JNMC, AMU, Aligarh
11 year old male patient with CAD (21? Ud1) had B/L SCPE. R-severe slip, L-moderate slip, R-C/R – C-Arm, both hips pinned in sits with cumulated concelleon screws.
2. Ilizaro Hip Reconstruction In Children – Series Of 9 Cases
Dr Nikhil Prakash Agrawal, Dr GS Kulkarni, Dr Ruta M Kulkarni
Post Graduate Institute of Swasthiyog Pratisthan, Miraj (Maharashtra), India.
In the pediatric age, there are various pathological conditions affecting the hip joint leading to severe pain, limp, limb length discrepancy, instability and disturbed hip and knee biomechanics In such circumstances, where femoral head salvage procedures and total hip replacement are beyond limits, Ilizarov hip reconstruction procedure provides relatively stable, mobile, painless hip with restoration of hip and knee biomechanics.
Material: In our institute at Swasthiyog Pratisthan, MIRAJ, we have performed Ilizarov hip reconstruction in 9 pediatric patients in the following hip pathologies.
1. Old infantile septic arthritis of hip - 4 cases. 2. Unreduced old hip dislocations – 3 cases. 3. Idiopathic Chondrolysis – 1 case. 4. Perthes disease – 1 case.
All patients were evaluated on basis of clinical symptoms – hip pain, limp, shortening etc. Clinical sings like hip and knee range of movements, trendelenburg lurch etc., and radiological sings. Age group ranged from 6 to 12 years.
Method: Ilizarov hip reconstruction is a Pelvic Support Osteotomy procedure with two level osteotomy. After Girdlestone excision of femoral head, proximally subtrochanteric valgus and extension osteotomy is done which supports against the pelvis. Distally corticotomy done at supracondylar level which permits lengthening and varusisation to correct proximal valgus and balance the mechanical axis of limb. Stabilization of the osteotomy is done with Ilizarov external fixator.
Results were evaluated on basis of residual pain in hip, ROM of hip and knee, trendelenburg lurch, shortening etc. We obtained excellent to good results in 7 cases and fair in 1 case, 1 case is under observation. All patients had significant relief of pain and lurch in hip decreased by almost 70%. All patients had good range of motion at hip and knee joints allowing them to suit cross-legged and to squat.
Discussion:The magnitude of such anomalies may not be very great when considered in comparison to other affections of the musculoskeletal system. Still these are important. The study results are comparable to other studies but a single study insufficient to answer all the questions and more similar studies are required to substantiate any of the above statement.
Conclusion:We conclude that Ilizarov hip reconstruction procedure performed over pediatric hip offers a valuable and effective surgical modality preserving hip mobility, stability, correction of shortening, decrease of abductor lurch and well aligned knee.
3. Management of Grossly Displaced Compound Grade – Iii Surpacondylar Fracture Of Humerus In Children With Cross Pin Fixation – Lession Learnt
Dr Vipul Shah, Dr JK Jain, Dr UB Yadav, Prof. AN Vamla
Department of Orthopaedics, MLN Medical College, Ahmedabad
Displaced supracondylar fracture present varying arrays of complex problems in management, the addition of compounding adds yet another sinister dimension to the problem and bring in its wake multiple management dilemmas.
Material and Methods:Twenty one cases of grossly displaced compound Grade iII supracondylar fractures in children were evaluated between Jan. 2002 – July 2003. The wounds were debrided and the neurovascular status assessed. Two brachial artery injuries with distal intact capillaries were pinned without repair. In one case repair with sephanous vein graft was performed. Cross pin fixation was performed in all cases. One preoperative radial (nerve) palsy, was observed, which recovered spontaneously.
Results:The results were assessed according to the criteria of Flynn et al (1974). There were 18 excellent results (85.7%), two good results and one poor result (4.7%). There were no fair results.
Keywords:Cross pin fixation, Internal fixation, compound supracondylar fracture.
4. Primary Management Of Idiopathic Clubfoot By Ponseti Technique
Dr Nikhil Prakash Agrawal, Dr GS Kulkarni, Dr Ruta M Kulkarni
Post Graduate Institute of Swasthiyog Pratisthan, Extension area, Miraj – 416 410 (MH)
In the early 1940s, Ignacio Ponseti developed non-surgical approach for the management of clubfoot and he is rightly considered as the “Living God” of clubfoot treatment. It consists of gradual gentle manipulation and serial plaster casts when the child presents very early, preferably in the first week of life. This allows relaxation of collagen and atraumatic remodeling of joint surfaces without fibrosis and scarring resulting from the surgical release.
Material:Since 2001 in our series at Swasthiyog Pratisthan, Miraj, we have treated 36 dub feet in 29 patients. Bilateral deformity seen in 7 patients and unilateral deformity in 22 patients. 20 Boys and 9 girls were affected. Average age of presentation was 3 months (fn?»m five days of age till six months of age).
Method:Caws, adductus, varus, equinus (CAVE) which are the components of clubfoot deformity are all corrected simultaneously, except equinus which is co~last. Elevation of first metatarsal and supination of forefoot corrects cavus. Simultaneously the whole foot is gently and gradually supinated and abducted under the talus while applying counterpressure against lateral aspect of head of talus correcting metatarsal adductus and heel varus. Equinus is corrected last by progressively dorsiflexing the foot after the varus and adduction have been corrected. However, to facilitate more rapid correction, a percutaneous tendoachilles tenotomy is done in 97 to 99% of patients. Correction is maintained by toe to groin plaster cast with knee in 90-dregee flexion. Usually 8 to 10 serial casts correct tile deformity. After that foot is splinted continuously – for three months and during night for three to four years to prevent relapse.
Results:Full correction by Ponseti technique achieved in 32 cases. Percutaneous T A tenotomy performed in 99% of patients. Recurrence and secondary survey were required for following cases
- For equinus, percutaneous tendoachilles Z plasty done in 1 case.
- For adductus correction tibialis anterior transfer done in 2 cases.
- Releapse occurred in 1 case (due to late presentation) for which RPMR was performed
Ponseti’s non-surgical management of clubfoot deformity is the best. Safest and highly effective treatment modality, which has minimized the use of surgical management and the associated morbidity resulting from extensive release.
5. Remodeling Following Fracture Tibia And Fibula In Children
Dr B John, Dr Amitabh Dwyer
Spontaneous correction of residual angulation occurs after union. This is because the physis responds to malalignment by differential growth, which tends to align the diaphysis perpendicular to major joint reaction forces. However, remodeling of tibial fractures is often imcomplete. We attempted to define the critical acceptable deformity following fracture shaft of the tibia in children which remodels satisfactorily. Forty eight children in the 3 to 12 years age group were followed up clinico- radiologically over a period of 10 years to analyze the correction of deformities following fractures of the shaft of tibia.
Seventeen children with isolated fractures of the tibia had an average increase in limb length of 8.9mm, 23 children had an average shortening of 11.9 mm at final follow up. Anterior angular deformity corrected maximally (66.2%), followed by varus (53.2%) and valgus (35.8%) deformities. Posterior angular deformity were 120 and 60 respectively. Realignment of a maximum of 100 varus and 50 valgus to normal physiological configuration of the tibia was noted in the coronal plane. Up to 5 of rotational malalignment was noted initially which did not change at final follow up.
6. Secondary Treatment By Mcmurry’s Osteotomy (31-05-02) & Hip Spika (14-06-02) Which Also Failed
Dr. S K Singh
Ortho Spine & Joint Replacement Surgeon, Apex Hospital, DLW Hydil Road, Varanasi
Diagnosis?
7. Septic Arthritis Of Ankle With Distal Tibial Osteomyelitis Presenting With Calcaneovalgus Deformity
Dr PN Gupta
Department of Orthopedics, Govt. Medical College & Hospital, Chandigarh
Sequalae of septic arthritis and pyogenic osteomyelitis in children can be devastating if treated / detected late. Destruction of femoral head resulting, as a sequalae of Tom Smith arthritis is well known. Involvement of distal tibia is less common than proximal tibia or femoral involvement; the after effects can be equally serious. Unfortunately in India a lot of cases present late to the treating physician. One such case is presented.
Case Report:An 8 years old girl from Himachal Pradesh presented with progressive deformity of left ankle region since 5 ½ years. This deformity followed pain in ankle region at 2 ½ years of age and the patient had an abscess drained at local hospital at the ankle region. At presentation at the author’s institute, patient had calcaneovalgus deformity and scarred puckered skin on lateral side (Figure1). Radiographs showed partial destruction of distal tibial epiphysis (Figure 2).
Management plan:In the first stage the ankle is planned to be brought at the level of ankle mortise using distractors considering the poor skin on lateral side. In the second stage ankle fusion is planned. The patient may require further procedures for limb length equalization.
8. Surgical Management Of Displaced Supracondylar Fractures Of Humerus In Children: - A Prospective Study Of 33 Cases
Prof. Rajesh Kanojia, Dr Alok Sud, Dr Vivek, Dr Akshay
Lady Hardinge Medical College and Associated Hospitals, New Delhi, India
Keywords: Displaced Supracondylar Fracture – Children – Surgical Management
Abstract:We report the result of thirty three consecutive displaced supracondylar fractures of humerus in children (mean age 7 yrs) treated from Feb’ 2002 through June’2 03. Twenty cases of displaced supracondylar (simple) fractures were treated by closed reduction & percutaneous pinning under General Anesthesia & IITV. Thirteen cases were treated by open reduction and ‘K’ wire fixation (failed closed reduction and compound fractures). Open reduction was done by combined mediolateral incision to avoid scaring of intact posterior and / or anterior soft tissue. At the final follow up (avg 15 months) using FLYNN’S CRITERIA the clinical results were :
| Excellent | 52% | |
| Satisfactory | Good | 21% |
| Fair | 15% | |
| Unsatisfactory | Poor | 12% |
88% of cases treated by this protocol were free from deformity and regained good range of motion. The poor results were due to cubitus varus deformity (2 cases) and stiffness (2 cases). Majority of displaced supracondylar fractures have satisfactory outcome by this safe and efficient protocol.
9. Umex Fixature In Compounds #S Tibia In Paediatric Group
Dr KA Saindane, Dr NK Saindane
Suyog Hospital, Sakri Road, Dhule 424001 [MS]
Compound #s in children posses problems while treatment in the paediatric age group Implants are rarely used. Healing capacity is tremendous & remodeling is also boon for these patients, hence internal fixation is almost not required. Unique external fixation system called as umex is used in my study.
Material and Method:Total 36 patients were studies. Male: 23 Female: 13. Age distribution is from 5 yrs to 12 yrs Classification grade 1:21 grade 2:8 grade 3a:5 grade 3b:2
Operative Procedure:Debrided thoroughly removal of clots, foreign material, dead bone pieces, with ample normal saline, wound is washed. In safe corridor 2 mm k wires are introduced in uni planner fashion. # reduced and fixed with umex fixature. If possible wound is closed. Secondary debridement was done in three patients. Secondary procedures were done in three patients (partial thickness skin grafting was done in three patients) Removel of fixature was from 8 days to 21 days. AK cast was applied till bone heals.
Result:All #s were healed. Average duration for healing was 56 days. Non non- union was seen. Superficial infection was seen in 8 patients at the # site. No pintract infection was seen.
Discussion:This is novel method. It is light weight, easy to install, any peripheral ortho hospital# ends are realigned, compressed or distracted. Wounds are easily inspected local dressing can be done regularly. If required, secondary surgical procedures can be done easily. Limb elevation is easy. Early movements of adjacent joints are possible. Less trauma to tibia due to 2 mm k wires.
Conclusion:It is novel method, easy to apply with all good results in comparison to only pop cast.